Right Care seeks to be smart care.
In the first part of my career, I rarely looked critically at the evidence. I was too busy; and I was more trusting of the vertical hierarchy of medicine. Eminence-based medicine seemed normal. Listen to the experts, for they are experts, went my mindset.
Then something happened. When internal cardiac defibrillators (ICDs) came to be around the turn of the century, someone asked me to do a talk on ICDs. This forced me to study the actual data.
I’ve never forgotten what I learned–not merely about the studies, but also how device companies used key opinion leaders, free food, junkets, and selective reporting of favorable data to make their case. I watched, and lived through the irrational exuberance of ICDs. (That experience still stings the medical profession.)
That was the beginning of my skepticism. Although I am no statistician or methodologist, I now read past headlines and abstracts. I look for the “hidden stitch” in studies.
Here is a slide from the famous Stanford professor, John Ioannidis, in which he lists the biases that exist before a trial. Who knew? 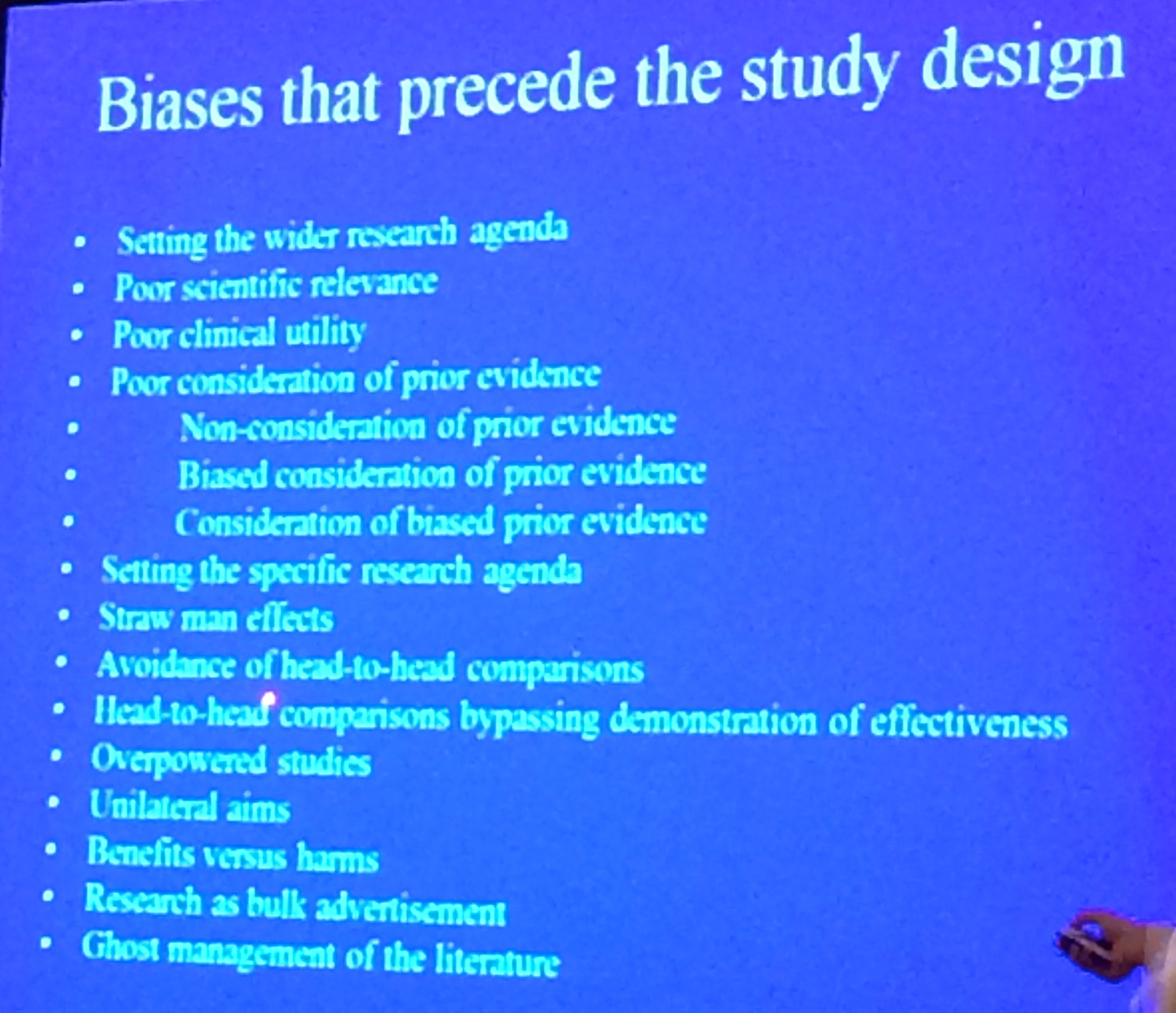
Then there is this picture showing how results from big data sets depend greatly on how one slices the data. (credit — Ioannidis)
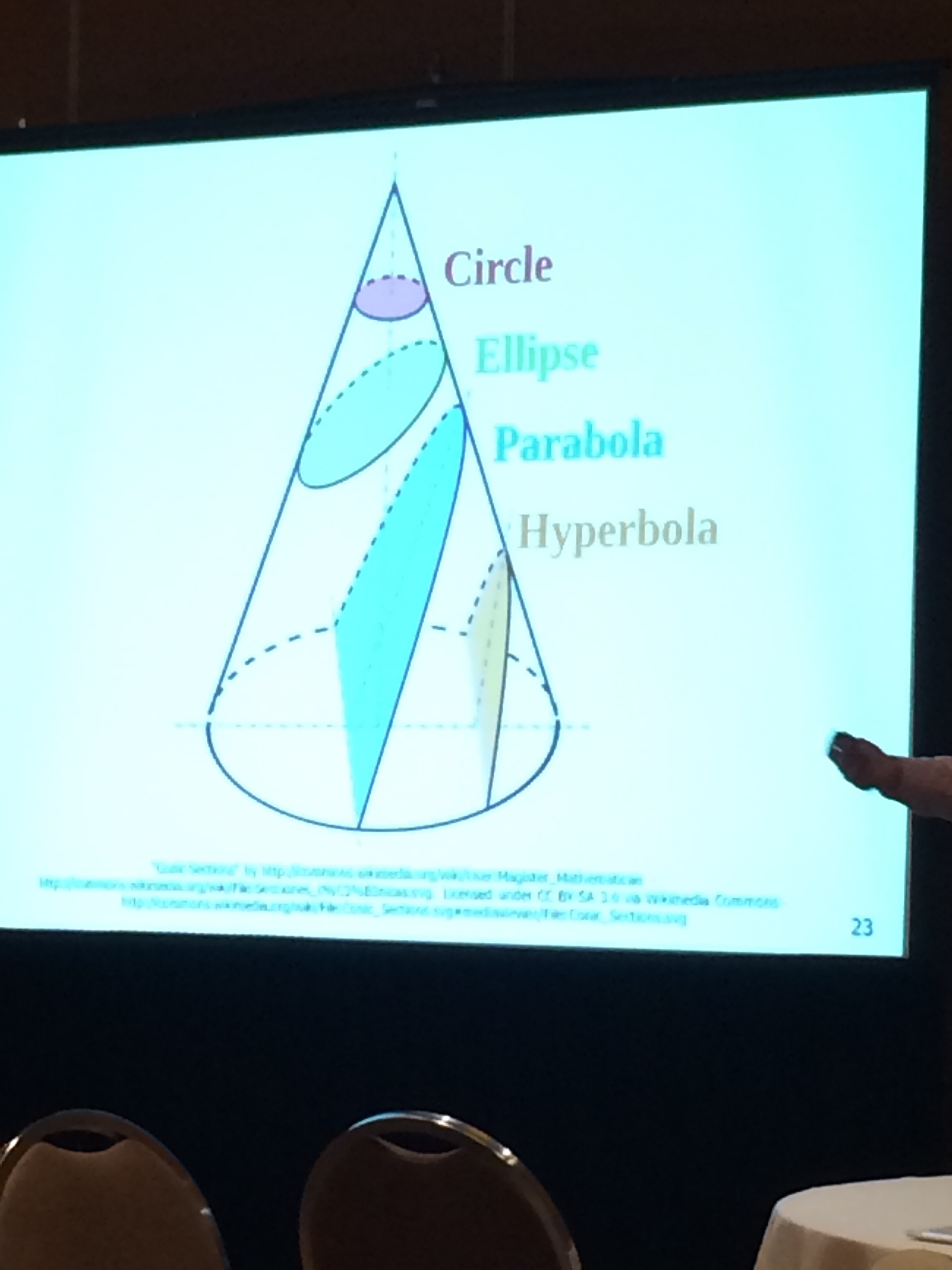
Pharma and device companies don’t stay in business unless they design trials and slice data in a way that favors their product.
But industry bias is not bad; it’s expected. Industry works in the healthcare system we have created. It’s our job to recognize that free samples, pens, burritos and CME aren’t at all free.
Dr Ioannidis explains more about bias and other problems with medical evidence in this famous paper…Why Most Published Research Findings Are False. Bias and flaws in methods do not only affect industry studies.
In the interpretation of medical evidence, Right Care practitioners look at Figures 1-2 or Tables 1-2 of major trials. These show the actual differences in events. The key word being actual–not relative. The actual difference is often tiny. A 30% relative reduction looks great but if the event rate goes from 1% to 0.7% the actual difference is not so much.
Right Care means skillfully communicating these numbers with patients. Dr. David Newman, an ER professor and methodologist, believes the best care happens when patients and doctors have the same data. He and colleagues have created a website called NNT.com. This website looks at actual data from clinical trials and calculates how many patients would need to be treated (or harmed (NNH) for one to get the result.
To be fair, others have criticized the use of NNT in explaining medical decisions. But I like the NNT and NNH because it helps me understand the magnitude of benefits and harms. And if I understand the actual data, I can better explain it to my patients.
Another example…The news yesterday was that the American Cancer Society decreased their support of mammography in younger women. Why? Because there is no evidence that screening mammography in this group saves lives. But there is data showing that it creates harm, in the form of overdiagnosis and overtreatment.
Right Care supporters knew the limits of screening mammography a long time ago. The delay in getting good information to women occurred because the dollar-infused pink forces swamped the voices of reason.
Right care stands against hype. Right care seeks to understand and recognize bias, to frame decisions based on evidence not eminence, and most of all, Right Care is candid about uncertainty.
There is a lot of uncertainty out there. In fact, the more I learn, the less certain I become.
JMM
Right Care needs more voices. Go visit the Right Care Alliance. And speak up.
2 replies on “Right Care Action Week — Be skeptical”
I’ve mentioned before that one of my relatives received a needless, harmful pacemaker through coercive malpractice, and was left to live with the consequences. Now, an octogenarian relative with iatrogenic heart failure from recent treatment for advanced cancer is getting a CRT … with defibrillator. He’s never had a ventricular arrhythmia, and his LVEF is middling. I can just imagine the poor man getting the standard spiel: “You don’t want to diieee … DO YOU?” “Oh, no sir, never….” I can only hope that the 33% rate of tricuspid valve damage will not soon become the next thing that is killing him and simply must be aggressively treated.
[…] RightCare Action Week—Be Skeptical—Dr. JohnM Blog […]