I am in San Diego to participate in the Lown Institute Road to Right Care: Engage, Organize, Transform conference. It is an honor to be included in a conference that has “right care” in its title.
Tomorrow, Dr. David Martin (Lahey Clinic) and I will co-present a case-based session on the overuse and misuse of AF ablation. We will talk about the drivers of overuse, including the confusion about the disease AF, the fee-for-service system, our culture of doing, and the if-you-build-it-they-will-come model of hospital growth.
The tide is changing in how doctors think about AF. Mainstream electrophysiology now gets it: AF is a symptom of a systemic disease. Take a look at my report from the recent Western AF symposium.
We used to see AF as its own disease. It was in a silo. The new knowledge that AF is a symptom of widespread cardiovascular disease disrupts the status quo. It also means the right treatment of AF is rarely doing more damage to the atria with ablation.
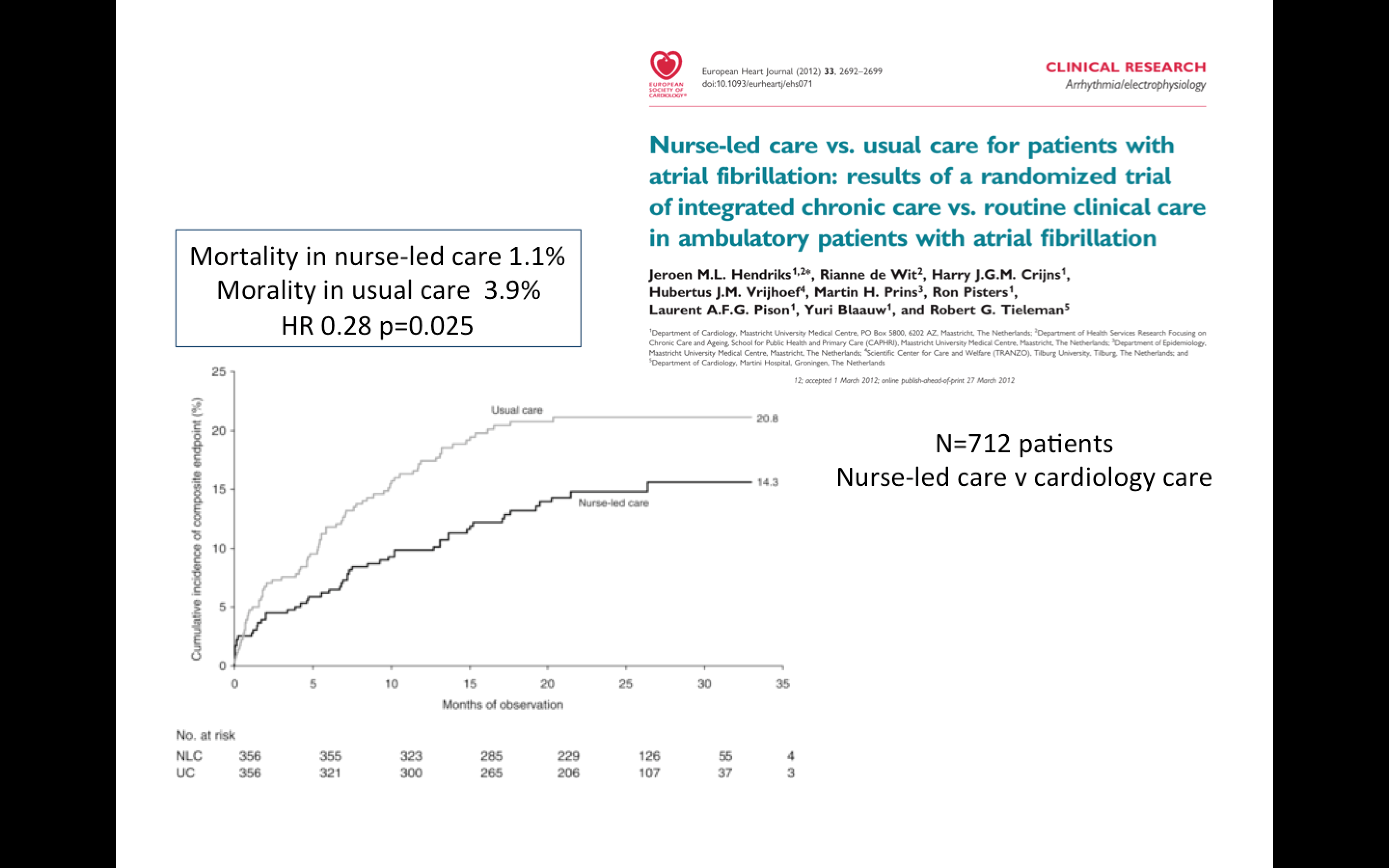 If we in the US really cared about delivering the right care for patients with AF, we would pay more attention to the work Dr. Jeroen Hendriks, formerly of Maastricht University, Netherlands, now in Adelaide Australia. His team of researchers showed that nurse-led care–aided by computer algorithms–in an integrated clinic improved outcomes.
If we in the US really cared about delivering the right care for patients with AF, we would pay more attention to the work Dr. Jeroen Hendriks, formerly of Maastricht University, Netherlands, now in Adelaide Australia. His team of researchers showed that nurse-led care–aided by computer algorithms–in an integrated clinic improved outcomes.
Here is a presentation from Prof Hendriks. Yes, he said nurses were in charge of the AF clinic, and this nurse-led team care trounced the usual care from cardiologists.
I met Dr. Hendriks at the ESC conference in Barcelona. I reported on his study for the Trials and Fibrillations column on TheHeart.org
The superior performance of a nurse-led AF clinic makes perfect sense. If AF is a symptom of widespread disease that stresses the atria, the right care is to treat the source of distress to the atria. In the US, this usually means treating high blood pressure, high inflammation, diabetes, obesity, sleep disorders, psychosocial stress and alcohol excess. None of these conditions get better with a catheter.
To be sure, there will always be a role for skillful catheter ablation in the left and right atrium. Just not as much as is being done now. Too often, AF ablation is not the right care.
JMM
13 replies on “The right care for patients with atrial fibrillation”
What about those of us with perfect health (including good diet, right amount of exercise etc. )other than atrial fibrillation? I searched and searched for a way to resolve my afib without an ablation. I would love to know the underlying cause of my afib as I am a huge believer in addressing causes. If all of one’s other heart measures look great, blood pressure is fine, not overweight etc, what is the likely cause? For me, ablation 4 years ago gave me back my life.
Hey Lisa, yours is a good question–and it gets to the classification of AF. There are patients, perhaps like you, with a focally-driven source of AF. It is almost like an SVT. These patients respond well to ablation. Focal source – focal treatment. But this scenario is rare. Most patients in the US do not have this kind of AF.
Thanks, Dr. John!
I saw Dr Martin at Lahey in 2011 for my (Lone??) paroxysmal AF. Say hello for me.
Dr Martin passed me along to his associate, Dr Bruce Hook for consideration for an ablation. I’ve had three ablations with him. I’ve felt that I’ve been taken good care of each time, but now questions arise.
To what degree are arrhythmias subsequent to PVI (with cryo) iatrogenic?
Is the spreading of “do less” philosophy being appropriately accompanied with a “do more” approach with respect to lifestyle coaching and other interventions for before-the-the-fact AF prevention? For before-next-time prevention?
According to what I’ve been told, I have no risk factors.
Perhaps all risk factors are not known?
Perhaps there are factors that are a risk for some and not others? (Personalized medicine)
I set up a medscape account when you started referencing it for some of your articles.
But now they are refusing my login, and I am completely baffled re: how to get the account straightened out.
Is there a way you can reference your pieces with going through Medscape?
Very encouraging findings. I have no afib risk factors; not overweight, BP is WNL for a woman my age, non-smoker, no sleep apnea, good diet…except off-the-charts stress levels the past two years and most likely a ton of inflammation to go with that stress. Throw hormonal changes into the mix, and I’d say we have a winner.
I love the shift away from RX/procedures and more toward addressing lifestyle factors. When I discussed my stress level with the docs in the ED while in Afib, one of them looked at me and said, ‘You’re lucky this isn’t an MI.”
Since then, I’ve taken my foot off the gas and with the exception of the occasional “blip” things are good. Unfortunately, the docs out here are all about search and destroy medicine. I know my body well enough to know what my triggers are. Anything to stay out of the ED or even the doc’s office at this point. You need to have a talk with the docs out this way for sure. (Orange County, CA) The local hospital has a shiny new ablation center, and they are really selling people on it; hosted patient luncheons and all. Terrifying on many levels.
Not so terrifying when it’s the only save you have left… and it works.
Much depends on the skill of the doc doing the ablation. None of the docs out here have the level of training/experience that I would trust for myself or a loved one. If someone is lucky enough to find a highly skilled doc with the right experience level (has spent enough time in the EP lab) then that’s great.
Obviously ablation is a highly personal choice. For me, however, the thought of someone either freezing, burning or otherwise altering my heart tissue/pathways is terrifying, especially in light of the statistics that point to the need for repeat procedures or “touch-ups” As you know from your experience, anytime there is general anesthesia involved, there is risk. Anytime a doc works with the heart, there is risk. I’m glad it worked out well for you, but it’s not something I have a lot of faith in at this juncture.
I was like Lisa in that I was perfectly healthy, no risk factors. I spent eleven years doing everything I could to adjust my lifestyle for the better to avoid my episodes. Believe me, it was no easy thing to make the decision I did. I knew most of the risks. you can never know them all. As it was, cryo PVI left me with phrenic nerve palsy for half a year. It was alarming to have half a working diaphragm. At the time.
Anything rather than the Quality Of Life ruining AF.
True, I had the Lahey Clinic an hour away.
I was diagnosed with AF and Type II diabetes in July 2014. It was a wake up call for sure but all is going well.
The most significant decision to support better health was to retire. In October 2014 I retired after 30 years in health care. I loved my work but had noticed that I was not enjoying it as much as I had over the years and I also noticed that I was most likely to experience AF symptoms at work. It was a great decision and I am loving it! I also have not had any symptoms since my retirement.
No doubt the medications and my physician’s care are part of feeling better. However, until I was retired I wasn’t really aware of how stressed I was.
For some, at least for me, there is a vagal/esophageal connection that I’ve never gotten a good answer to.
I’ve gone 2 years between episodes, and the last time a year and a half. In all cases, it starts in the middle of the night after extreme GERD and stomach bloating. Once it starts, there’s no stopping it without a cardioversion. No drug will bring me out of it, and taking a rhythm control med is pointless as a preventive. In between those long spaced out episodes, minor intestinal or esophageal problems will trigger some PVCs or extremely short tachycardia runs, but no major episode. It takes a whopper to get it going. The last episode occurred after having a healthy dinner that included beans and a big salad. The resultant gas and GERD set me off at 3am.
I have recently started seeing some research studies done on that interaction. Up to now, my experiences with this connection had been brushed off, and generally dismissed in the available online materials I had found.
Some aggressive surgical intervention was suggested early on, but I wonder if any type of ablation would be helpful at all, and perhaps very counterproductive, given the nature of the trigger, and the infrequency of the episodes?
Hiatal hernia & AF:
http://www.medscape.com/viewarticle/759995_6
Thanks Jeff. That was one of the new studies I was referring to. I have a copy for my cardiologist printed and the link ready for his attention.