On Telehealth, an older couple asked me a tough question about COVID19. They asked whether this virus would either be gone or less dangerous in 6 months to a year.
It was a curious question. I replied, Why do you ask?
Doc, we have a big family with many children and grandchildren, most of whom live nearby. We miss them. We’ve been isolating, but it’s hard; we did it for 6 weeks. Doing it for a year or more would be miserable.
We saw on the news today that the battle with the virus would be long. A man called it a cruel new normal.
So doc, if you tell me the the virus will be gone in a year or it will be less dangerous to get infected later, then it makes sense for us to keep isolating. But if the situation will not be much different a year from now, we would just as soon see our family and take the risk. Of course, doc, we would still be sensible. We’d not visit if someone was sick; we would wash our hands and wear masks.
Indeed my patient was correct. Dr. Scott Gottlieb writing in the WSJ, did not mince words:
Hospitals and public-health systems will have to contend with persistent disease and death.
In essence, my couple asks whether flatten-the-curve policies save lives. Buried in that question are three other questions: namely, in one year, will the virus be 1) gone, or 2) less contagious, or 3) less deadly? If any of those three are true, then my couple could rationally decide to stay lonely for a year or more.
I study this new virus and this once-in-a-lifetime-situation every day.
I don’t think flatten-the-curve policies will change any of those issues. Let me explain my reasoning. I may be wrong; tell me if you disagree in the comments.
Flatten-the-Curve Purpose
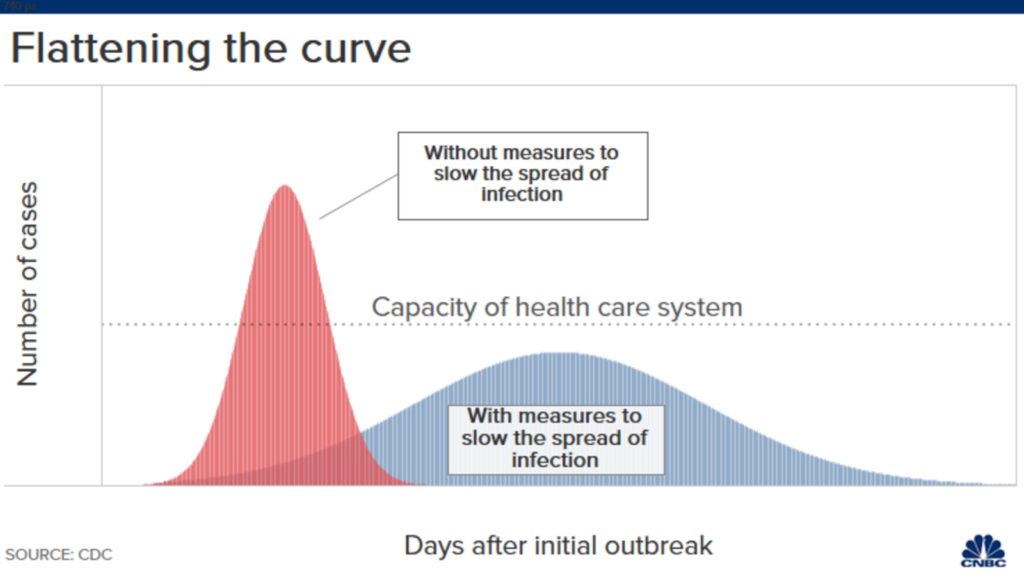
You now know the famous curves–one with an early surge of disease, and the other flatter curve that spreads the infections over time. The y-axis is number of COVID19 cases.
In early March the COVID19 narratives were from Wuhan, Iran, Lombardy and Spain, places where surges overwhelmed hospitals. In the US, COVID cases spiked in NYC.
Early COVID19 surges were over-running some big-city hospitals. This was bad because it caused excess or preventable death–people who could have been saved were not saved because of shortages of ICU beds, dialysis equipment, staff and ventilators.
Social distancing policies and postponement of elective medical care were necessary to stop the excess deaths. These policies allowed time for hospitals to prepare for COVID19 cases and for doctors to learn how best to treat these patients. Exhibit A: not intubating patients early.
Social distancing worked. The number of cases slowed and the US got into the blue part of the curve. But now, months later, the narrative has changed.
Change in Flatten-the-Curve Narrative
What was once flatten the curve to prevent over-running hospitals has changed to flatten the curve to save lives. Some likened moderation of social distancing to human sacrifice.
That change in framing, I believe, is misleading. I will argue that the cumulative deaths from COVID19 will not be reduced significantly by flatten-the-curve policies. And that this virus will be as dangerous to vulnerable patients in 6 months to a year. We should be allowed to debate this.
My case has eight assertions.
First: the virus will not be contained. The chance for containment has long passed. The virus transmits before people know they have it and many patients never develop symptoms. It will be with us until an effective vaccine is both widely available and widely used. (See #6)
Second: Tests will under-perform. The high rate of asymptomatic disease, the low sensitivity of PCR tests (false negatives), imperfect specificity of antibody tests (false positives) and concerns over privacy mean that we should expect less from test and trace–even if proposed by a Nobel Laureate. Carl Bergstrom and others write persuasively on major barriers to contact tracing in the US.
Third: US hospitals are now prepared and in little danger of being over-whelmed. In fact, many hospitals are so dormant they are nearing financial ruin. Healthcare workers have been furloughed due to postponement of elective work. I’ve talked to numerous colleagues in the US and the message is clear: hospitals are under-capacity and prepared for a “persistent†number of COVID19 cases during the coming months/years. Hospitals now have COVID response teams.
Fourth: Americans are not stupid. Before governors enacted lockdowns, economic activity and travel slowed, the NBA, MBL, NHL stopped their seasons and medical meetings were cancelled. People socially distance not because police are bearing down on them, but because it makes sense. The pictures of spring-breakers in Florida and crazies-with-guns in state capitals bring clicks to news organizations but belie the majority of sensible people in this country.
Fifth: Public-health surveillance has improved. Tests may underperform but they will not be useless. Tests will help signal coming hot spots and that will allow communities to act locally. Other technologies may emerge that help prevent surges. One cool example is the use of resting heart rate apps that might signal health officials early on.
Sixth: (I need a few paragraphs): Social distancing will not lower the infection fatality rate or IFR. Remember the red and blue curves? The y-axis of that graph is number of infections. Due to the contagion of this virus, the area under these curves is likely to be the same at the end of two years. Ok, then, if the number of cases is similar at two years, then the number of people who cumulatively die will not likely change either.
The only way fewer people die from COVID19 over time is if the IFR declines. Here is where American exceptionalism misleads people. Politicians have a strong bias to pump up optimism on any potential medical advance–no matter how dubious. (Exhibit B- hydroxychloroquine.)
That is not how Medicine works. History is replete with examples showing that drug development is super hard. But leaving aside the challenge of developing new drugs against a new virus, the basic math of COVID19 creates a huge barrier for success: already, more than 99% of people infected with this virus survive. A therapy that has a massive 50% reduction in death from a disease with 1% mortality (high estimate) delivers only a 0.5% absolute risk reduction.
What about Remdesivir? This antiviral may help a little. But even if you believe its ≈ 3% reduction of death was not due to chance (p = 0.06), the death rate in the remdesivir arm in that trial was 8%. Remdesivir is no game-changer.
COVID19 vaccine development is sobering. Most experts say a safe and effective vaccine is at least 18 months away. Again, the 99% survivability erects a huge safety barrier for vaccine makers. (I get that from Dr. Paul Offit.) Given society’s tension over vaccines, it would take only a tiny signal of harm to derail a coronavirus vaccine.
A slight hedge on the sixth assertion that IFR remains constant: some smart people say that getting the virus later may be better because doctors will be a little better at treating this disease. For instance, a year from now we may better understand how to use drugs that block clotting; we may have better vent protocols. These are big ifs. They may drive the IFR down a little but IFR is already low. Another benefit of infection in a year would be that most hospitals will likely allow family visitors.
Seventh: The more we test, the lower the IFR goes. Early estimates had it at 3%. Then it was revised downward to about 1%. Now most people put it at 0.1-0.5%. But that is still quite serious. You’ve probably read that 0.1% is similar to flu mortality. That is likely wrong. Dr. Jeremy Faust points out that flu mortality is grossly overestimated and is probably much lower than 0.1%.
Eighth: I wrote a piece on Medscape about the harms from COVID19 interventions. One of the points I made is that right now we count only deaths from COVID19. We stay riveted on day-to-day numbers. But the endpoint of this crisis is not next month but in 1-2 years. And when we get there, we have to count people who died from COVID19 and those who died from other causes.
This preprint from prominent researchers suggests a substantial proportion of excess deaths observed during the pandemic are not attributed to COVID19 and may represent an excess of deaths due to other causes.
In my column I cited an older study by Raj Chetty and co-workers that finds a strong association of lower income and lower survival. And that is the rub with COVID19 interventions: they make poor people even poorer. The rich just work from home. It is possible, therefore, that our social interventions will be especially hard on the disadvantaged.
I realize that no person overtly dismisses the harm from economic shutdowns. My friend Dr. Dan Morgan expresses my frustrations well in this thread. Why can one safely critique a drug for COVID19 but not massive public health interventions?
Conclusion:
I did not have a clear answer for my couple. But after thinking and writing about this question it seems that the most reasonable approach in this crisis is transparent information–no matter how stark. And, crucially, we must have space for public debate.
I hate this virus. I wish it never came. But we can make it worse by avoiding hard discussions on tradeoffs, the limits of modern medicine and risk.
JMM
P.S. At 173 comments, I cannot keep up the moderation. Thanks for your interaction. I have closed the comment thread.
187 replies on “Can We Discuss Flatten-the-Curve in COVID19? My Eight Assertions”
Did you see the May 3 episode of 60 Minutes? They profiled health care in rural Texas. Those people are so underfunded, understaffed, under equipped – it’s just tragic. Yes, hospitals in major urban cities are better prepared, but I think rural America is going to be hurt by this, especially the states that did not expand Medicaid. Public Health needs to be better funded and more attention paid to it in rural communities if we’re going to go for herd immunity. It appears that is now the plan.
I worked in San Antonio and we’d receive many patients from outlying community hospitals. My understanding is the hospitals are in rough shape under good conditions.
However, the cultural aspects of those communities, the people stay isolated. San Antonio has had a low count in COVID19 cases to date, hopefully it will stay that way.
Good point Allison. I hope this virus opens peoples eyes to The poor health and low wealth suffering caused by people in power in places like Texas. We need to stop the senseless greed, lack of compassion and prejudice of so many in this country.
Hi John – thank you for these thoughtful reflections. One additional rate limiting step that is a preventing a restart of the regular business of health care is the PPE shortage. Supply chains aren’t secure and this severely undermines the confidence of health care workers to do their jobs. Properly used ppe works to protect them and they will continue working while they have it. But I’m not sure I share your confidence that health care systems could not be quickly overwhelmed with unchecked spread. The difference between Canada and the US curves is solely (or at least largely) due to the timing of social distancing and other public health directives. And the vast majority of Canada’s first cases were imported from the US (not China or elsewhere). A few more weeks of exponential growth would (in my view) certainly have overwhelmed our system – depleted our ppe and led to many more preventable deaths. And, most importantly, it would have left us unprepared to look after STEMIs, strokes, and emergency surgeries. This may seem a bit hyperbolic but I think the math supports this prediction. A society cannot function without a health care system. The number of non-COVID related deaths would have been even higher.
Many thanks – I always enjoy your posts.
Chris, you mentioned one of my biggest concerns. Dr. Mandora, your argument is predicated on hospitals being ready to respond. I don’t disagree on that per se, they have response teams ready, but they do NOT have the necessary equipment needed, mainly PPE, but also testing and the necessities required there in. Without the massive amounts of equipment that is needed, we are putting our most vital workers in more danger and could easily overwhelm a lot of hospitals. We need to find a happy medium between stay-at-home orders and a complete return to previous practices, but we are not ready to do so until we have the equipment needed to best fight this.
Apologies, Dr. Mandrola; I massively typoed your name in my previous comment.
That is not universally true…at all, really. The PPE situation is MUCH, MUCH improved, to the point where many med device manufacturers that switched their manufacturing to PPE now have large inventories sitting around because healthcare systems and states have stopped purchasing it.
In my own experience, we have plenty of PPE. I have never gone without (even though, many shifts, I have gone without enough patients to support hospital operations…censuses are so low).
There are probably some focal hospitals with shortages, though even residency friends in NYC report having enough PPE now, but, currently, it is not a universal problem and definitely not a reason to stay closed, IMO.
Finally, I think the country, government, healthcare systems have had their eyes opened wide with the initial shortage and now have experience with scaling up production should it be needed in the future.
Thank you for speaking the truth. People seem to line to just spew misinformation to make a point. We’re not experiencing any shortage of PPE whatsoever, nor is my cousin who is a nurse in Boston. The PPE shortage is a complete myth.
So the personal accounts of doctors and nurses who say that they don’t have enough masks or gowns are myths? Sorry, but your personal account and the report from Boston don’t convince me.
Mike, I live in the Detroit area and in the hospital where my father was, they were sanitizing and reusing their masks, as recently as last week.
I will have to disagree with you on the PPE. I work in a rural hospital in Louisiana and we definitely have a shortage of certain items. The most important item is N95 masks. We cannot get our hands on the ones we have been properly fit tested for, so we use what we can get. The PPE that we can get, we’re paying top dollar. What cost $6 in February, now cost $60 or more. If you know of someone with an abundance of PPE, specifically N95 mask, please send to small rural Louisiana.
The people in our rural areas of Texas are in some instances at zero infections. What data shows the possibility of these small rural areas being overwhelmed? As stated in another post, many sicker patients travel to the larger cities for care anyway. Are you actually a longtime resident of Texas? It seems you don’t have a sense of how our medical system functions.
I agree. As a lifelong resident of a rural Texas town, our county has totaled, to date, 7 covid cases. Currently three of those have recovered (so you can get a sense of how late it was before we had any positive cases).
People that live in rural areas are choosing to live in rural areas the same as urban dwellers choose to be urban dwellers. The nature of rural living is a completely different creature and cannot be compared to that of a city. Like a previous poster mentioned, we stay somewhat isolated naturally. We do not have to come in as close contact with people as ones who live in a city do.
I quite agree with you, John. The goalposts of Flatten the Curve have been moved, and I’m not sure I agree with the new goals. Like you, I don’t think the virus can be contained, so bottling it up at great cost only delays sickness, but does not prevent it.
It was reasonable to do everything when growth in cases and deaths was exponential, but we’ve gotten off that curve well over a month ago. Now that growth is NOT exponential, it is quite easy to model, and the healthcare system is nowhere near capacity. In my own hospital we are at 60-70% capacity, whereas on a normal day, we never fall below 96% capacity. Every day I see people who should have been treated a month ago.
My only caveat to your comment is that your and my hospitals are at 70% NOW. With elective surgeries canceled, and people avoided hospitals due to virus fears we have no problems dealing with COVID patients. My concern is that when everything opens back up and we are running at 100%+ with everyday health issues that we will again dip into the territory of excess deaths related to the virus due to taxed resources. I don’t know what the answer is as the economic impacts thus far have been just as devastating as the virus. I hope that hospital administrators and emergency operations teams are planning for the surge of COVID patients that will be stacked on top of our normal case loads. Wishing you the best.
I understand that from larger hospitals. But I work in a rural, critical access hospital. We have been shut down from making any money through this….let me explain. As a county facility, we don’t make a profit. But we struggle every year to stay afloat. With the shut down of elective procedures, we are cutting hours of staff in all departments. We have purchased so much more PPE than ever. We have had a very low census on the med-surg floor. And if things don’t pick up soon, we could close. We are the only facility in a 25 mile range. That could amount to a lot of deaths for our own county. We are about as prepared for COVID as possible, test a lot and so far have done well. We have a huge geriatric population, so deal with influenza all the time, as well as COPD, etc. I don’t want to have any death. But would hate for a lot of our “regulars” die because we were closed.
You need to mark every hospital entry, procedure, and death as Covid. FedZilla is reimbursing from $13,000 to $27,000 for every covid patient. NYC hospitals are doing it.
Seems to me you are saying lie! It doesn’t matter what they are admitted for – it must be COVID!! That is why the numbers are so wrong! Dr. Brix has already said that even if they dies of pneumonia without being tested it is still a COVID death. No – it is NOT. Let these small hospitals open up and begin moving again. The virus isn’t leaving us anytime soon but a lot of hospitals will!
That is a lie.
Any hospital in a county with a population density less than 5,000/square mile should be back to no restrictions on procedures. The curve has been flattened and there is now plenty of PPE. People have to be smart about how they interact and their personal hygiene.
Curious where you are with a hospital census still that high. In my area, even lab techs are being furloughed because census is so low. The delay in cancer diagnosis and treatment will have consequences for some patients.
I wonder when the baseline true data in stating cause of death will start when states reopen so we get an accurate measure.
Looks legit to me.
In terms of the couple, I’d be curious if they had to visit a hospital, your thoughts on scheduled antibody testing (conferring immunity) in conjunction with nasalpharyngeal swabbing (active colonization) or staff to insure safety of patient population during the resumption of normal hospital functioning.
Have you noted any published SOPs for hospitals or physicians to return to normal operation of admitting patients and maintaining a ‘gold standard’ of patient safety?
Thank you for your reason in this time of politicising the disease. I live in Sweden and there is a fight to get rid of the expert driven approach to get more political decisions. I myself trust our epidemiologists. Their strategy is only to take enough action to protect the health care. Our failure lays in not succeeding in keep the disease out of the residential homes.
I am somewhat gratified to learn that “politicizing the disease” is not a problem unique to the US. I wish you well in Sweden.
I agree with you in your basic position.
You did not emphasize enough, in my opinion, how the print and TV media dwell on all the personnel tragedy we can find in this pandemic without analyzing the situation in all its parts the way you have done.The media is highly critical of anyone or any body that fails to embrace any action which threatens the idea that the lockdown and its economic repression are the only acceptable approach to Covid-19.This is a tragic mistake because the media controls the debate.
Waiting for a vaccine before opening up the economy assumes not only that a vaccine will be developed , will produce an antibody response but also. that the vaccine will protect the most vulnerable who are known to respond poorly to vaccines and that vaccine deniers will accept the vaccine.
Stark public debate is, as you state, woefully lacking and essential.
So well stated
@William Reichert, Well stated. But one additional thought on the vaccine. How fast can it be produced? We in the US would need 330 doses just for our country. That is double what is produced just for the normal flu. But the entire world would need a vaccine and many of the ingredients/production capabilities are in various countries around the world. As a reader states, NZ would want to vaccinate their entire population to make sure their total shutdown effort was worth it. Your point in addition to the large quantities needed make the vaccine a further off solution than many are hoping.
Good thoughts but mutation is probable how can you stay ahead. why not work on nutritional immune systems for long term protection.
I agree with the sentiment that the media is controlling the debate. In the U.S., that’s a function of the media being mostly headquartered in New York City, which has been the hardest hit. It only makes sense that news anchors there would know someone either at their media company or in their neighborhood who has Covid 19 or who has died from it. That, then, drives the narrative for the rest of the country. “Why are people on the beach, when they should be locked down?†It is also a narrative driven by people who have full time jobs with health insurance who can neither understand nor appreciate Americans’ anxiety about “getting back to workâ€.
I also agree with the good Doctor. I think Americans are savvy enough to know whether they want to be in a crowd (I don’t), whether they need to wear a mask (I do) and how best to live their lives while understanding that, with this disease, we need to maintain distance and wash our hands regularly. I’ve treated this like a flu season on steroids. But I am still willing to get a haircut and go to my gym (whenever both of those are open again).
Well Said. I know no one really understand this virus fully. And I think we are not taking into account the real human life of the lockdowns such as reduced or delayed cancer screenings, abuse, etc. which dont show up in the models.
An excellent and sobering analysis
Delaying Covid infection has value:
Israel isolates coronavirus antibody in ‘significant breakthrough’: minister
JERUSALEM (Reuters) – Israel has isolated a key coronavirus antibody at its main biological research laboratory, the Israeli defence minister said on Monday, calling the step a “significant breakthrough†toward a possible treatment for the COVID-19 pandemic.
The “monoclonal neutralising antibody†developed at the Israel Institute for Biological Research (IIBR) “can neutralise it (the disease-causing coronavirus) inside carriers’ bodies,†Defence Minister Naftali Bennett said in a statement.
The statement added that Bennett visited the IIBR on Monday where he was briefed “on a significant breakthrough in finding an antidote for the coronavirusâ€.
It quoted IIBR Director Shmuel Shapira as saying that the antibody formula was being patented, after which an international manufacturer would be sought to mass-produce it.
The IIBR has been leading Israeli efforts to develop a treatment and vaccine for the coronavirus, including the testing of blood from those who recovered from COVID-19, the respiratory disease caused by the virus.
Antibodies in such samples – immune-system proteins that are residues of successfully overcoming the coronavirus – are widely seen as a key to developing a possible cure.
The antibody reported as having been isolated at the IIBR is monoclonal, meaning it was derived from a single recovered cell and is thus potentially of more potent value in yielding a treatment.
And delaying also has severe consequences that will increase world poverty and increase deaths by other causes. This is not a binary choice!
https://www.lohud.com/story/news/coronavirus/2020/05/08/nys-covid-19-deaths-top-20-000-race-ethnicity-risks-unresolved/3090578001/
We are finally getting data on who is actually dying and why lock up aren’t stopped the spread. 98% of hospitalizations with underlying heath issues.
Congratulations on that thoughtful and rational way of thinking!
I still have differences on point seven. If seasonal influenza virus have less virulence than SARS-COV-2 is something yet to be proved. Let’s remember that we have vaccines and antivirals for this virus and people are still dying from it.
As you concluded, we need to think and make decisions with real un-politicized facts and not with fear. Tradeoffs are needed to be done. We, as a society, are obligated to assume some risks (0.1%) and work our asses off to found a way to diminish the IFR. COVID19 is here to stay.
I believe that anything other than a full re-opening of society immediately (with older people and people with underlying health issues isolating, etc., as they are doing now) will lead to more deaths (not Even counting death from affects closing down). Reason: given how fast and how transmissible this disease is, if we fully opened up we would have or nearly have something approaching herd immunity within six months. Dr. John‘s patients will then have considerably more safety and going to visit their family, or people in the hospital. Without opening now, I think it is reasonable there will be a much bigger second wave in the fall and winter.
I respectfully disagree. I think there is a misunderstanding and underestimation of the impact of flattening the curve by most people. It has been sold as solely a strategy to give the healthcare system time. I’ll make a point it is a lot more than that.
Your point 1. This might be the case in places like NYC with a 25% IGG+ rate. It is not the same across US or in other countries. Suppression strategies can still be implemented successfully on a regional basis. Several countries have suppressed the virus.
Your point 2. I think prior evidence form South Korea, Taiwan, HK, NZ, Australia and Norway all prove this works and can be done with good results even if tests are not great. I do think it would be much better it testing performed well, but all countries that suppressed the virus relied on test and trace strategies. I live in Brazil, and we are constrained by limited testing. I have proposed I different approach. Isolate all suspected cases individually (if this sounds too much, consider an entire country stopped instead of the 1% suspected). Do surveillance tests to monitor positivity rate aiming at very low. Do not use tests to guide isolation or quarantine, neither in nor out. Probable symptoms isolated for 14 days. Contacts traced and quarantine if possible individually, if not as a family, but tracing symptoms to direct to individual isolation. Increase sensitivity by not testing even if intervention (isolation + quarantine + tracing) overused.
Your point 3: agreed for most of the country in the US, but not for many places here in Brazil. To me healthcare is not a metric to release extended social distancing, but a metric to start or enforce it.
Your point 4: depends on your population and how much distancing is needed. If crazy as NY or Milan at peak you need aggressive measures. If not social distancing is not binary and can be tuned to individual responsibility and flexible measures if system well controlled (mostly by r/t and other transmission measures)
Your point 5: to me tests are (A) PCR used for surveillance of the outbreak by test positivity ratio if a scarce resource or a diagnostic tool to count cases. All probable cases should be isolated regardless. Can be useful if available to reduce isolation if improved symptoms and 2xPCR negative (not a local reality to me).
(B) Serology: used for epi evaluation of community spread and immunity information (questionable). I do not think we can act upon such tests on an individual level.
Your point 6: as I stated above, I think there is evidence to suggest flattening the curve does more than delaying cases. You can suppress the virus completely. Also, Chinese data clearly demonstrate reduction in CFR (IFR can never be measured) but the test and trace strategies. Cases are identified and admitted earlier, making support interventions more effective. You do not only reduce mortality, but also CFR with a comprehensive strategy.
Getting the virus latter might also be better beyond the idea of better medical care. Most virus mutate and less lethal forms are likely to survive and develop more, so latter forms might be less aggressive though this is still unclear.
Your point 7 underestimated IFR. In NYC the mortality is already at 0.14% though not all had COVID19. So IFR cannot be lower than this. Since serology still positive in only 25%, even if sensitivity is low, IFR has to be at least 2 or 3X more than 0.14%. It might even be 4-5X larger. That would be 0.28% to almost 1% in a city with a median age 2 years younger than average US. Since age is the main driver of death, US death could be even higher.
Your point 8: Not much to discuss, final results can only be estimated when this is over.
As requested, none of the arguments are political, I do not even live in the US, so your politics do not really affect me, but we have similar discussions in Brazil.
I am also glad to hear rebuttals to the above.
Marcio, you are misrepresenting the numbers in NYC. There was a 25% antibody rate an entire month ago! In addition, studies are showing that in many cases, people who have had the disease (and lived) are only 50% likely to have detectable antibodies. In other words, up to 50% of NYC one month ago could have already had the virus.
Age is not a risk factor. Only 6% of hospital admissions for the virus in NYC were for people without a serious underlying condition. Please stop spreading lies.
The current (this week) rate is 20%, with a larger sample.
I haven’t heard the 50% antibodies claim — no way 50% of NYC has antibodies.
Marcio, thanks for your detailed analysis of the article and hit the main points well.
I strongly agree with your comments on the fatality rate. By the most optimistic calculations, I come up with a 0.5%-0.8% rate. This is further supported by the recent statistical studies of excess deaths which show a considerable under-counting of Covid-19 induced deaths around the world. The only studies I’ve seen which indicate death rates lower than this are the biased and flawed studies like that on Santa Clara. No good science supports the lower rates.
https://www.google.com/amp/s/medicalxpress.com/news/2020-05-team-covid-infection-fatality.amp
.37% in German study
@Ted-san:
You write: “This is further supported by the recent statistical studies of excess deaths which show a considerable under-counting of Covid-19 induced deaths around the world.”
Dr. Mandrola directly addresses this claim in Point 8:
“This preprint from prominent researchers suggests a substantial proportion of excess deaths observed during the pandemic are not attributed to COVID19 and may represent an excess of deaths due to other causes.
In the places that have “ended†their outbreak (there is an excellent article in NatGeo about NZ), they have done so at tremendous cost to their economy. They better understand the concept of taking one for the team and have much less wealth inequality, so they will recover together much better than the US. Also, it’s much easier to isolate an island nation (no planes or boats in or out, done). BUT, there economy is very dependent on tourism, accounting for 6% of GDP and nearly 8% of the country’s workforce. They will eventually have to open back up, and they will only delay their ongoing outbreak. This virus is global. This virus is established in most parts of the world. I personally think this is going to remain present going forward, and will become the “other, more virulent influenza.†They have to face their infections eventually to get to herd immunity.
Great comment. I will say though, that “taking one for the team” is all fine and good if you are talking about having less clothes, cheaper meals, a smaller house, a worse car, etc. But what about the additional DEATHS that economic downturn causes for others? Even if they care for one another (which is great and everyone ought to do) giving to charities will drop, meaning more people around the world will starve or not get live-saving medical treatment. And that’s just a start.
I think it is unwise to look to China and cite their data and mimic their response(s). We know much of what comes out of China is untrue.
Age is not a risk factor. Only 6% of hospital admissions for the virus in NYC were for people without a serious underlying condition. Please stop spreading lies.
Hi, I have to agree with most of this. It was quite thought provoking. The one thing that I may disagree with is that hospitals are prepared. However, it is really easy to overload the hospital systems in urban areas. For example, in my county, it takes only 0.02% of the population needing ICU care at the same time for all ICU beds to be full. The county has almost 2 million people & could easily be the next New York. It’s something I think about as an ICU nurse. I think there’s a balance that needs to be found, but it is difficult to balance between a rock & a hard place.
Oops! I meant to say that I disagree that hospitals are completely prepared. That really depends on the size of the surge we get.
So why have hospitals failed to prepare?
I would dispute your first assertion that the virus will be with us until an effective vaccine is widely available and widely used.
I would assert the virus will be with us until herd immunity is achieved. A vaccine is merely a tool/vehicle to achieve herd immunity.
I am concerned that too much hope is being held out for this magic bullet which may not be so magical and may not come for a long time if ever.
The ideal vaccine is a close enough approximation to the virus to generate an immune response without causing the actual infection.
Well if 99% of people have a medically manageable/not serious illness and up to 50% of people have virtually no symptoms, why are we so afraid of the illness?
We are afraid because of the risk of contagion, infecting our vulnerable loved ones. If we can protect the vulnerable while allowing the other 99% get infected, we don’t need the vaccine.
A criticism against this approach is that just because you are infected does not mean you are going to be immune. You could get infected again. Well this argument is an even stronger one against a vaccine which is an impostor.
I think we need to double down on our elderly and vulnerable. This includes any healthy young subjects (spring breakers) who live with or may otherwise expose the vulnerable. The rest of us should be allowed to carry on and be progressively exposed to work on building up herd immunity.
Secondary waves will be inevitable if we don’t develop herd immunity which will take longer if we keep social distancing and people do not get exposed.
Viruses will always be with us. And death will always be with us. That being said, our focus ought to be on increasing 3 things: personal vigor, personal hygiene, and civic duty.
Personal vigor would consist of a concerted prolonged effort at improving behaviors conducive to obesity reduction(the primary COVID risk factor no one seems to want to touch) and the reduction of co-morbidities. So, yes; exercise, nutrition, stress reduction.
Personal hygiene. Basic hand-washing, hand-mucosal contact reduction, clean up after yourselves(toileting behaviors), coughing behaviors. Clean up after yourselves, soap and water simplicity.
Civic duty means being concerned with your neighbors, co-workers, friends, the postman, team members. If you’re sick, stay home. If you have to go out, personal hygiene rules apply. With extra precautions, maybe that means a mask; not my rules, but common sense and the application of a morally and ethically informed personal liberty.
No one wants to touch the obesity issue because it’s not actionable in the short term. Long-term it looks the the elephant in the living room.
This is an unfortunate consequence of living in the era of “you be you.” The Oprah generation. The costs to the US can be directly attributed to that poor advice, along with one of the biggest crimes against humanity – the USDA food pyramid that was taught in schools for decades.
It’s a complicated issue & argument. But doubtlessly as our medical industrial complex has grown into a behemoth, our personal *health* care has withered, outside the elite?
ASM to that. The food pyramid was an outright lie, propaganda by the meat and dairy industries.
I see what you did there
Ha.
These are my thoughts exactly. I think we need to focus on making ourselves healthier, practice common sense personal hygiene, and do our personal part to stop the spread of disease, just like any other disease. We don’t need these overblown and draconian measures and we can’t keep shutting down for every new disease that comes around.
Great article addressing something we are dealing with right now. We live in Israel. The country has a done a great job at flattening the curve and is now removing a lot of the restrictions. I’m 61 and my wife is a little younger but with some medical history which puts us both at slightly higher risk. In addition to grandchildren, we also have two younger children who still live with us. So this balance between our risk and giving them freedom is huge for us.
One thing you didn’t address is the possibility of herd immunity. I’ve seen in several places that the R(0) value is around 2.5, if so, herd immunity could be reached at around 50%. Once we flatten the curve in various places and start opening up, more people will get infected. As our information improves and higher risk people take greater precautions on their own, we could reach herd immunity faster and with fewer deaths overall.
Simple question about testing for the antibody. Testing has been conducted for a few weeks now. I am currently waiting for my results. I read mixed feelings toward the accuracy of the test and if in fact the antibody protects you.
Is there any case where someone had it and it then got it again? If not wouldn’t that suggest the presence of the antibody is effective? Your thoughts.
I love your well thought out article and feel the same way. I am in the higher risk group and would love to see my grandchildren. I
Not to answer this question, but I will say that I am constantly stunned at the numbers of testing being presented in the media. My husband and I are both respiratory therapist (I am not currently practicing), and he has had known exposure to two pulmonologist that were sidelined with Covid19. My husband had repeated chills, etc., but never any fever, and has thus been denied any test. We finally stopped asking. We quarantine within our home, because I am higher risk. Our governor was on TV today touting that we have some of the lowest infection rates in the States- but, I have talked to endless people that can’t get tested, no matter how easy they say it is to get tested. The only exception I have found to that is a local MD that is offering an ‘antibody’ test, that in the small print asserts that ‘it is for Corona Virus- not specific to Covid 19’. A non-medical person will likely not understand the significance of this disclaimer. This should be illegal- because anyone who has had had most colds will have antibodies for Corona Virus, and happily skip away thinking they are immune to getting Covid19 ‘again’- when they may have never had it in the first place. Physicians that are offering these generic antibody tests should stop this, unless they have an antibody test shown to be extremely successful in Covid19 identification, or this will merely propagate the spread.
I am curious how many SARS-CoV-2-specific And SARS-CoV-2-specific-antibody tests are available? Are a majority of testing places using these specific tests? Or are a majority of tests only generic Coronavirus tests?
Great write-up John. I have been following you on Twitter and have greatly appreciated your insight and others I see commenting with you. Continue the good work.
You analysis largely leaves out an analysis of increased hospitalization rates by focusing too much on the total death rate. Flattening the curve is also useful since it buys us time to find a vaccine. That’s not to say a complete shutdown is the only way to flatten the curve, but infection delayed is valuable in that it may be delayed beyond vaccine. Viewing only death rates, however misses other side effects from this virus such as reduced lung capacity and potentially reduced life expectancy after having had this… The jury is still out on these issues… .1% of the US population is still 330,000 people, which is in the ballpark of WW II. .3% puts us at a million dead. Of course those numbers would be reduced by those that don’t get the virus. Those are staggering numbers. As of today, we’re about 1/5th the way there, yet there’s no wide-spread evidence that 1/5th of the whole US has been infected (just in the hot spots). So given the deaths we’ve seen to date, .1% seems awfully optimistic at the end points… The New York serology numbers suggest many times that (since if you take the population, multiply it by the percentage the population of NYC and use that for IFR the math works out to between .6% and .8% for the error bars in the population estimate). So even the back of the envelop says we need to take things to reduce the R0 of this thing, like social distancing, masks, testing and tracking and cancellation of huge gatherings. Whether it merits more draconian measures is a political question, but just going back to work is not going to have results significantly different than what happened in NYC, which will be quite bad as exponential growth will soon take us from ‘excess healthcare capacity’ to a system that’s overloaded.
So three points: it’s more than just the deaths, it’s worth blunting the spread and infection delayed potentially is infection prevented by vaccine or rendered moot by improved treatment (not a sure thing, true, but also not 0 chance).
Hear here!
Comparisons with wars are extremely misleading because they completely ignore the huge demographic differences between those who die in combat (median age in 20’s in most conflicts) and those who die from COVID-19. The median age of the latter is in the upper 70’s in the U.S., looking at CDC information that shows fatalities by age bucket ( https://www.cdc.gov/nchs/nvss/vsrr/covid_weekly/index.htm ). That’s not to say that the latter should simply be ignored. It is to say that any sort of reasonably cost-benefit analysis of public policy takes into account years of life lost in acknowledging that extending the life of people in their late 70’s is not the some as extending life of generally healthy people in their 20’s.
“but just going back to work is not going to have results significantly different than what happened in NYC.”
I strongly disagree with that for numerous reasons.
First, “just going back to work” is an unrealistic straw man, as Dr. Mandrola notes in point 4. Actual experience will include a measure of voluntary social distancing that wasn’t present in NYC, including both how people choose to interact as well as various measures taken by companies for workplaces.
Second, NYC is a huge outlier in the U.S. in some ways highly likely to facilitate the spread of COVID-19. General density is one, and I’ll particularly highlight the massive use of subways and trains. The NYC subway system has average daily ridership that’s an order of magnitude more than the #2 U.S. system (the D.C. Metro). Commuter rail (combined total for Metro-North, LIRR, and NJ Transit) is similarly over 4x ridership of the next biggest system (Chicago’s Metra). In both cases, the numbers drop even more as we move from #2 metro area farther down the list.
I live in a hipster-rich neighborhood of South St. Louis. Currently, it seems that the predominant attitude is “you should wear a mask so that I will never catch anything ever again, and I need to go to Home Depot to get some string trimmer line because I’m bored to death during Staycation.”
St. Louis City currently has 71 dead, out of a population of 318,000 – 0.02%, just a little bit higher than our casualties from our ongoing gang and drug wars. What I’ve been hearing at work is that a large number of the victims are from nursing homes. And on the way home from work tonight, I saw a Metro bus pulling into the front of a large state-run residential mental health facility. Boy, this all makes perfect sense… sigh…
Me? I’m an essential old fat man in a retail job, and I think I had it back in January. According to the hipsters, I should be dead by now.
I would kill for a cold draft beer in a frosted mug with little chips of ice floating on top of the head, with a nice bowl of pretzels and peanuts off to the side. You know what that would taste like? Freedom.
I live in New Zealand. Because this country was following science we have 21 deaths total. (Compared to almost 70,000 in the USA — our population is about 1/80th of the USA so our total would equate to if there were only 1600 deaths in the USA.) I am an emergency physician and I don’t need to go to work every day fearing bringing it home to my family. There is a hell of a lot less pain and sorrow here thanks to flattening the curve.
Your argument overlooks what happens if a vaccine is developed 6 months from now, so we all get vaccinated and then the curve never rises here in New Zealand. I think all this social distancing will have been well worth it. And we will have saved tens of thousands of lives.
@Mark Sagarin – New Zealand didn’t “flatten the curve”. New Zealand has suppressed the disease because there was a small enough number of infected people that was possible. That’s of course desirable if possible / practical.
Dr. Mandrola makes the claim (in his first point) that the U.S. – like most countries – is past the point where containment is possible. I agree with him.
Looking at hypotheticals, I also have strong doubts whether containment over the medium-term would have been possible in the U.S. even if the CDC and local health authorities had managed to contain the disease in February. Even if the U.S. shutoff legal travel indefinitely, hundreds of thousands of people illegally cross the U.S. southern border each year. They then disperse to several metro areas in the U.S. and often live in relatively crowded conditions. There’s no evidence to date that’s been a significant vector for spreading COVID-19 in the U.S., but it seems a near certainty that any globally prevalent disease with these characteristics (particularly spread by mildly symptomatic and asymptomatic people) would eventually reach the U.S. by this route.
I’m also surprised that a physician thinks that development and widespread deployment of a vaccine within 6 months is a plausible timetable.
Doc:
Do you think that you will keep the island nation of NZ closed for 1 year, 2 years, 5 years before you allow outside people to visit without quarantining the visitors for two weeks?
And once you stop the quarantining of new visitors/tourists [5 to 7% of your economy], do you think that NZ will not get another case of Wuhan virus?
And then if you do get another case of wuhan, do you shut the country down again?
I would like to make a comparison. When you are overweight and you realize this is a serious health problem for you, you can either start a hard restrictive diet, lose weight quickly, stop the diet and take all the weight back ( and even more) in a very short time. On the other hand you can institute a new way of living with different habits, cutting a little on sugar and unhealthy food, star exercising a little, lose weight les drastically but not put it back on again. Covid 19 will have us induce long term changes in our way of life by becoming part of our environment the same as HIV did or the flu did after the 1919 epidemic. Vaccination will be a part of it but probably no magic bullett. So be prepared for some permanent changes, if only washing your hands more, coughing in your elbow, use tissues and take good care of your elderlies and neighbours. Maybe wear face masks on certain occasions ( public transport, senior homes, large gatherings) Just my 2cts.
Thank you for writing this, I enjoyed reading it. Do you think that one of the reasons the flatten the curve narrative has not changed is money? Right now every country in the world has opened their pocketbooks and while medical teams are working together on a treatments and vaccines, at the end of the day they are competing for money and to be the one that “wins†(I.e. Gilead). A return to a new normal has the potential to limit what is currently unlimited funding, therefore experts are pushing a wrong narrative as long as they can, knowing at some point the economy has to reopen. Curious on your thoughts.
I don’t know. But the tension b/w moderating the lockdowns and accepting an increase in viral cases has become politicized. As a doc I simply approach it as 1) there is a disease (virus), 2) there is a treatment (lockdowns) and both have harms. In Medicine it’s crucial to consider both. The public debate, IMHO, focused much more on the harms of the virus rather than harms from the intervention.
Thanks for posting this. I don’t have any medical or epidemiological training so I can’t critique your assertions. I am interested to see if anyone seriously challenges them, though. Best regards from Owen Sound, Ontario, Canada. P.S. Have you ever cycled the Dolomites?
Interesting article. It’s sad you have to tell people not to post hateful replies!
Here is my question. The flu obviously comes back every year… some different strains; some maybe the same. But other big viruses do really die out in a year or so (SARS, H1N1, Spanish Flu). Why do some die out and why do people think Covid 19 will not?
I wish there was better reporting on the ages of those who have died and the existence of underlying conditions. I think that is very relevant. There is a little bit you have to dig and you can only find it some places. I want to understand better the risk to healthy people.
John I’ve heard a lot of discussion from folks trying to attribute many additional deaths to COVID though not confirmed. I have no data or information to validate and would trust that those who do would be far ahead of me without me throwing undue speculation around. But some of the points you made in your 8th assertion are what make me have a gut feeling that many of these deaths are not from the virus itself but unfortunate side effects. For example, people in rural area or lower income areas that already had less access to health care maybe have even less now in addition to fear of even seeking medical care. It would seem logical that there would be a significant number of deaths for these reasons as people with completely non COVID related issues either delay or fail to seek timely medical care resulting in unfortunate fatalities. Have there been any reputable papers written on the subject you could recommend.
I’m a civilian, and some of these numbers are overwhelming to me, though the sense that I’m getting is that we’re at a point where we have to realize that this, as a previous commentator has pointed is out, is like changing the word diet from a verb to a noun. This makes sense to me. I watched the previous news conference by our Governor (I just moved from NYC to ABQ) and she kept saying that we will have to move forward in a Covid-19 world. We have to take tentative, slightly-risky first steps to see if we can exist in this world together with it and everyone else in a way that minimizes damage. She even acknowledged that her advice was contradictory, essentially, “Don’t leave the house, but also spend money at your local retailors.” I’m all for these grandparents being able to look at their life and say, “This is the amount of time that I have and I want to spend it the way that I want to spend it and I’m willing to take my risks.” This is a sensible choice to me and it’s their choice and their risk, so I’m all for that. There was a commentator who said that they want to drink beer in public, and I can totally understand that feeling. I love going to a bar to have a good burger and a beer. I’d love to do this, but to do that (or for the previous commentator to drink their beer) then someone I don’t know would have to take risks. I know that this comment should be about the article, and not about the comments, per say, but for every person who just wants this to stop so they can spend time with someone else, there’s at least some amount of people who want this to stop so they can patronize shops. I see this situation like smoking (an admittedly hyperbolic analogy). The grandparents are aware that what they are doing is dangerous and could potentially be dangerous to others, but they are mitigating that with gear and distance. People who just want to patronize stores are asking the employees to light their cigarette for them and to sort of remain close-by them while they smoke it. And I know that the economy dying is bad for people. But it makes me sad that we always talk about problems of poverty as though we didn’t, essentially, create them. We were beavers who dammed up the river and then forgot the dam existed and started calling the river a lake. Beavers need that environment to live, we did not, but we did it anyway and it made life easier. Now, it’s under threat and instead of supporting those less fortunate or admitting that we sort of painted ourselves into a corner, we just keep saying, “But we need money.” No, we don’t. We need Food, Shelter and Water. You just can’t have any of that without our dam– I’m sorry, I meant to say money. Thanks for the numbers and the thoughts, and I think they can certainly help people make the proper choices for themselves. I just hope that these numbers aren’t used to force others to do things that just actually aren’t safe for them to do. Staying in can cause problems, but being forced to work also causes problems and it turns out that not everyone is that loyal to a McDonalds (a job that many admit won’t pay you enough). And your argument seems to be about making medical choices, but it will be used to determine economic ones. I can understand that, but that doesn’t mean that it sits well with me or that I want to participate in someone else’s economic choice. I don’t have to be involved in their medical choice and that would be weird. This one feels weird too.
Dr John, I think you pretty much nailed it. A few thoughts though. I do agree with you that theoretically, the area under each curve is the same, so the number of infections and death should be near the same. But flattening the curve does save us from excessive deaths due to lack of health care when our hospitals are overwhelmed, as you mention. Have to balance that with the fact that social distancing, unemployment, poverty also increase the mortality rate. Also, some predict a 30% rise in suicides to all of this. The potential for death related to these other causes could exceed those due to lack of healthcare if we did not flatten the curve. So we might actually end up with more dead if we continue these lock down policies for too long. Second, stretching this out makes sense only if you can get a vaccine ready in a short period of time or we can develop successful treatments that save lives. Well, even 18 months is probably not realistic for a vaccine, but even if it was, that is still too long to have an effect on our current problem. A vaccine only makes sense if this is going to be a seasonal issue. While we are learning a lot about treating this disease, we are not having a huge impact on mortality and likely will not. Third, a lot of the mortality we have seen in this country has been from elderly in nursing homes. With all of this social distancing, we have done a horrible job in protecting our most vulnerable. So continuing the lockdown vs opening things up in my mind doesn’t matter as much as doing a better job of protecting our most vulnerable. We have to do a much better job of this.
As far as the IFR, I find it much better to look at total deaths per population, since we don’t really know the true number of people infected, we just guess at that. So with influenza, the US deaths have varied over the past several years from a low of 12,000 in 2011-12 to a high of 61,000 in 2017-2018. That puts the death rate in the population somewhere around 0.015% annually. IF the estimates this will kill about 100,000 Americans are accurate, then it is still about twice as deadly as the flu. That stinks if you are one of the 100,000 (a friend and colleague is one of those) but still just a small fraction of our population. And if lockdown is not going to significantly change that number, then we should end the those policies and try to find a new normal going forward.
I agree with most of your assertions. The ethical issues need to be considered also. The severe COVID-19 cases disproportionately affect, poor people, people of color, and the elderly, as do many diseases in America. The IFR in people of color and poor people is shockingly high. See Navajo Nation statistics. Let’s review the ethics of calmly talking about IFR, when we know that rich people will not have the same risk of dying as poorer people. I cannot calmly accept that the fatalities over the next 2 years will be the same. More poor people will die. Best practices and availability of healthcare affect survival rates. I do not have a solution, except an overhaul of healthcare.I refuse to accept injustice and inequity.
I agree with you! This is a much broader issue and it is easy for people with affluence to feel more entitled to getting back to normal. What can we do to change such a broken system? I get so discouraged by the divide in our country and that a large number of people seem to be so self serving and refuse to see all the inequality that has been happening for a long time.
Likewise, the lockdown disproportionately affects poor people.
Thank you for your post. I am not a Doctor but if Hydroxy cuts IFR in half, why isn’t that significant?
Rusty — thanks. There is no evidence that this drug works. The early studies that suggested it might work were terribly and fatally flawed. To date, the available studies that have been published show no convincing evidence for HCQ efficacy. There are ongoing larger trials that will report better today soon. I don’t think they will show an effect. But we shall see.
Thank you for your article, it is thought provoking and shares a harsh reality. We are all going to have to adapt, personally and professionally. It is a shame that there are those who will have to live more of a changed life than others, given there age and health issues. My concern is for the minority that will not adapt, and perhaps cause unnecessary risk towards others, but again, the majority must be prepared. I would appreciate your insight, as to how and why South Korea seems to have achieved “successâ€, in keeping the virus at bay, and what steps could we have done differently (granted we must move forward, not backward).
Thank you
I have worked as a nurse in skilled care for 51 years I find it tragic that our seniors have not been given choices with quarantine they are being isolated in Senior Communities and Assisted Living violating their rights as citizens of this country. There is no option for them with decisions made for them. The instructions to wear masks is confusing for the general public when the CDC and Surgeon General provide opinions of the value of a mask. Finally the primary physicians have lost a say so on how their patients are treated holistically. But apparently journalist and politicians all have the tail wagging the dog. Finally on Nurses day I am sick of hearing about the fear we have in caring for patients with life threatening illness this is what we do and the less drama from people without studies in science the better.
My question goes to your first assertion. Given it’s asymptomatic spread; do you think containment in the US was ever possible.
Covid is like termites. By the time we knew it was a problem, it was too late.
I agree with your statement, “I realize that no person overtly dismisses the harm from economic shutdowns,” but I think it’s also true that these considerations haven’t been analyzed or at least discussed as much by the media and our policymakers. We hear from the epidemiologists and the public health “experts” all the time but we’re not having daily economic briefings, people aren’t considering what is likely to happen globally with regards to poverty, malnutrition and other diseases of the poor. Our economy makes up about 1/4 of GDP. Assuming we were the ONLY country locking down, that would be a bad recipe for the developing world. But it’s really the entire world shut down and this lockdown result in a humanitarian catastrophe. Nobody is doing that kind of modeling. At least nobody the media is paying attention to.
We never should have shut the economy in the first place. The tragic mistake we made was not better protecting those most at risk. 40 to 60% of ALL deaths worldwide occurred in nursing homes. Everyone likes to attack Sweden, because they were smart enough not to ever shut down their economy, so they never have to worry about a second wave. Let’s look at Sweden’s numbers. They have almost 3,000 deaths (50% in nursing homes) or 291 per thousand. The US is 218. The huge difference is according to Sweden’s population surveying, they are approaching 30% of their population with antibodies, the US has 5 to 10% at the most. If they achieve population immunity with 60% they will have 6,000 deaths (6 million infected) or an infection to mortality rate of .1%. If 80% is required there will be more deaths but the .1% stays the same. The University of Washington model just revised Sweden’s death toll down by 7,000 and will continue to do so. Even WHO is praising Sweden and told other counties they should do the same. The only way forward is to let those who are not at risk go back to work and school, lockdown those most at risk especially the nursing homes which is the low hanging fruit and instruct all those with underlying heath issues to stat home and wear a high grade mask in indoor public places if they need to go out. We need to follow the data and the science the quit the panic and the craziness.
The assertion that is most questionable is “Americans are not stupidâ€â€”I do not say this condescendingly. Rather, the stupidity is a function of the psychology of mass communications. The good reason for imposing lockdowns was to reduce excess mortality from overwhelming hospitals. However, the message from public health and state and local governments has conflated this rationale with how lockdowns reduce near-term total mortality. There is little dissenting medical opinion presented at the upper levels of the government response. For example, please name a respected expert who has disagreed with Dr. Fauci on important matters related to managing the pandemic. Even if you can name one, almost no average American can. Thus, Americans now broadly believe that lockdowns are the best response to the pandemic, period. When pressed, they may fall back to the test-and-trace prescription, which is just a closet lockdown position, for the reason you state: T&T is unlikely to be feasible in the US at this stage of the pandemic.
We need to turn the tide of propaganda-induced stupidity. One idea: an Oxford-style debate between Fauci and an expert with some important opposing views. I nominate you, but please feel free to pass the buck on to someone you think even better qualified.
Dr John- You make some excellent points, especially the point that this virus can’t be contained and is not going away. We need to learn to live with it. The best news is we know who is at risk. Sadly the more we try and contain it, the longer it will be with us. My poor parents are in quarantine for the foreseeable future and the economy is wreaked. It didn’t need to be that way.
We never should have shut the economy in the first place. The tragic mistake we made was not better protecting those most at risk. 40 to 60% of ALL deaths worldwide occurred in nursing homes. Everyone likes to attack Sweden, because they were smart enough not to ever shut down their economy, so they never have to worry about a second wave. Let’s look at Sweden’s numbers. They have almost 3,000 deaths (50% in nursing homes) or 291 per thousand. The US is 218. The huge difference is according to Sweden’s population surveying, they are approaching 30% of their population with antibodies, the US has 5 to 10% at the most. If they achieve population immunity with 60% they will have 6,000 deaths (6 million infected) or an infection to mortality rate of .1%. If 80% is required there will be more deaths but the .1% stays the same. The University of Washington model just revised Sweden’s death toll down by 7,000 and will continue to do so. Even WHO is praising Sweden and told other counties they should do the same. The only way forward is to let those who are not at risk go back to work and school, lockdown those most at risk especially the nursing homes which is the low hanging fruit and instruct all those with underlying heath issues to stat home and wear a high grade mask in indoor public places if they need to go out. We need to follow the data and the science the quit the panic and the craziness.
One thing that doesn’t seem to be well known to the public is that deaths are a lagging indicator to spread.
I’m a data analyst and from the data available in San Diego, deaths peaked and started falling at the end of march, suggesting the spread started falling at least the end of Feb.
I would also not use one lagging indicator for prediction so looking at the daily hospitalizations, I see a peak and falling 3rd week of march. Again suggesting spread had peaked end of Feb.
3rd lagging indicator is daily positive tests. If you normalize this graph for changing test parameters (increasing group size and number of tests) there is no peak but just downward trend since they started recording this data, again suggesting the the peak had occurred earlier.
A 4th indicator is a lack of indication. Schools closed here Mar 13 but we don’t see any effect on the other 3 indicators.
5th indicator is also a lack of indication. social distancing effects should have some effect by April 1st but even 6 weeks later we see no effects on the first three indicators.
So from a data analyst point of view we never had the ability to “flatten the curve” because the curve had come and gone before we realized it was here.
As I was comparing the daily death curves of Sweden which as you know did a much less draconian shutdown, to the US daily death curve, it follows essentially the same trajectory. Daily deaths are going down. I think in time, once Sweden reaches full herd immunity, which I have heard will occur in the next few weeks, their Covid-19 spreading will be very small while the spread in other countries will continue spreading until the virus is done doing its thing or a cure is found. I think when it’s all said and done, it will be obvious to all that Sweden made the right choice.
Assuming this is all true, what is the argument for any continued social distancing? Prolonging this for the sake of prolonging things when there’s real costs to doing so seems silly.
This is an excellent question and I would also like to hear the answer to. Maybe just to keep the serious cases below hospital capacity?
Hi Dr. John,
This is a well-reasoned argument and I think I agree with it generally. I would think that one affordable accommodation would be to identify the most effective mask for source control that can be manufactured for $0.05 and get everyone to wear them all the time everywhere they’re within 50 feet of other people out of their homes.
Far from giving people a false sense of security, masks are a kind of uniform that shows we’re all in this together and that this is a real thing, not just something in a TV drama, and also a good reminder not to touch our faces.
Even a modest reduction in R values would make this (I believe) the most cost-effective (and perhaps most effective in absolute terms) thing that we could do at this point. One wonders what would have happened if we had been able to implement something like this in January, or within a few days of some future outbreak.
One other thing: we should be doing quantitative PCR testing of viral loads in waste treatment plants on a daily basis. We’ve known for a couple months now that this is an effective wide-area surveillance method that costs virtually nothing and provides nearly perfect community sampling. More people should be talking about this.
Cheers,
Gavin
P.S. I just want to say that you and my other pandemic-era twitter follows like @AbraarKaran, @ProfDFrancis, @MicrobiomDigest, @EricTopol, @Toaster_Pastry, and @trvrb among others have given me restored faith in humanity and made me extremely sad I did not pursue a career in medicine when I was young enough!
Wow. That waste treatment plant idea is amazing.
Is there any published literature on that?
It could be a fantastic way to measure viral load in populations.
Google for something like: sars-cov-2 wastewater titer
First one I read was a month ago now: https://www.medrxiv.org/content/10.1101/2020.04.05.20051540v1
There’s been discussion, but I have not yet heard one political leader mention it. It seems like a solution to almost all the ongoing testing issues like sensitivity. For re-opening I think you really just need one thing, a measure of whether and how fast the virus is re-emerging, and this seems like the BEST way to determine that.
Dr. Mandrola, excellent analysis, and thank you for putting it together.
A couple of thoughts.
Several readers have comments on total shutdowns stopping the virus sold. But what will happen when their countries open? If New Zealand is able to get their country vaccinated in 6 months, as one reader mentions, yes they will succeed. But if not, they could easily still have many people who have yet to get antibodies through spread, and will start gaining in cases again. Singapore is a stark reality in what happens if you don’t stay shut down (especially if you have poor areas as they do with their transient workers). If a vaccine take 2 years to confirm and reproduce in quantities, these early wins may evaporate. What happens in poorer countries that cannot afford the vaccine in quantities and distribution immediately. Brazil is a prime example. They could shut down but be on the end of the vaccine distribution curve and it won’t matter. Africa and other poor areas could have this affect them for a long time to come. New Zealand is rich enough and small enough to be on the front of the vaccine curve and maybe it will work. So the vaccine effectiveness will depend on more factors than just a vaccine existing.
Your point #8 is right on point. I have been attempting to post and get correct statistics out and show where we cannot concentrate on the day/weekly/monthly stats but to look at longer term views back on the . The New York Times today did a piece on excess number of deaths vs. the average. The average will go up and down in the short term. A year from now the numbers will be totally different, but will scare people today if you only view short term statistics as they did.
Lastly, you have not made enough of concentrating on the three areas that are needed to be monitored and locked down in every country. The elderly (nursing homes etc.), people with pre-existing conditions, and lastly but most importantly the poor. The poor will have to work, may not be able to socially distance properly (due to high density living), stay clean (due to living conditions, homelessness etc.) or afford proper PPE etc.
Thank you again for raising up important issues that you have.
I recently read about a working group of critical care doctors at several hospitals who are developing protocols for C-19 treatment guided by their shared experiences. Among them seemed to be the beneficial use of anti-inflammatories like cortisone which reduces harmful immune response in the lungs.
Not that this is a game changer, but how likely is it that absent a highly effective antiviral, trail and error like this might lower morality in coming months?
Hello Dr. John, thanks for your article and thanks for allowing me to share my opinion. I will be brief and just say that the lockdowns must end. We cannot continue with this insanity. More lives will be lost to other causes than the virus if the lockdowns continue. I read in interesting article today on the negative impact on mortality of being unemployed. We cannot allow the continued loss of personal liberties, which are arguably unconstitutional. We were told that the lockdowns were to flatten the curve. That has happened. We know that the vulnerable need to be protected, so let’s do that and restore freedom to the rest of the country.
Sorry, but I find this article a total waste of time…
Please elaborate.
Thank you for your insightful, evidence-based article. I concur!
I would like to Point #9. Many leaders are not examining the allocation of healthcare resources, such as PPE. In Pennsylvania our Secretary of Health announced that PPE will be withheld from hospitals and shunted to long term care facilities. https://www.pennlive.com/news/2020/05/top-pa-health-official-says-state-wont-supply-masks-other-protective-equipment-to-hospitals-that-resume-elective-surgeries.html
The rationing of limited resources has grave potential to do much harm. Rationing can, in fact, be unethical and place an entire population of individuals who are not in long-term care at a serious disadvantage – with health care ramifications yet to be determined. It is unclear why the long-term care population is prioritized above others who are in also in need of life-saving and important healthcare services.
I would appreciate if these thoughts and ideas would garner some serious attention.
Could you address the benefits of social distancing and the use of masks when states open their economies back up? What effect would this have on the infection rates for everyone and the death rates for those over 65?
Even if my state no longer enforces social distancing or mask wearing, as someone over 65 with 3 bouts of pneumonia behind me and asthma associated with allergies, will it help if I continue to do both until a vaccine is available?
I hate to think I will have to stay locked down until we get the vaccine because I don’t think I can do it.
I am a pulmonary physician. I disagree with several assumptions. The first is that social distancing will result in the same number of cases, just over a longer period of time. If we look at the 1918 flu, cities like St. Louis had 1/8 the number of fatalities compared to Philadelphia although they were roughly the same population. This was attributed to different public health policies. Second, if we look at NYC, where the situation is the worst, the IFR is about 1%. That is if we accept the non-randomized antibody studies in NYC grocery stores that showed an antibody rate of 20%. That rate is probably high since shoppers at the selected grocery stores may have been more likely to have been. infected than those staying home. Anyway, if you do the math, New Yorkers who have passed represent 1% of the infected population. Secondly there is no historic precedent to show that any disease has infected the entire population of a country or the world. The goal of social distancing is to reduce the total number of those infected or who become ill. If we believe the China statistics, they were able to limit the number of those infected and those who died. We cannot engage in such draconian policies here, but we can look at Sweden compared to the rest of Scandinavia and conclude the Sweden’s policies have led to more death and more disease. Sadly, the lack of testing and personal protective equipment is what has allowed this terrible disease to spread. If the IFR is 1%, and we allow everyone to get this disease, we will be sacrificing about 3.5 million people. Finally, the early results from Oxford suggest that a vaccine may be available much sooner than anyone thought.
Dr. John, thanks! I agree with so much of what you have said. Three questions:
1) Do you have any suggestions on where to find analysis or studies dealing with the impact on world mortality CAUSED by an economic collapse?
2) Do you think allowing the majority of us (people who are healthy and young or young-ish) to get on with our lives could realistically HELP reduce the final death toll by getting us to herd immunity faster? (It might help to read my final question below to see where I am coming from here.)
3) What do you make of the fact that death from this disease occurs almost exclusively among the elderly and those with underlying health conditions?
Children & young adults are not at risk of dying, and 30 and 40 somethings are at practically no risk of dying either. (I mean “not at risk” the same way I would mean I am not at risk of dying as I drive to work, or my daughter is not at risk of getting kidnapped on her way to school — as in, it is so unlikely that it doesn’t paralyze me into fearful inaction, but I do take reasonable safety precautions for both.)
Shouldn’t THAT be a huge factor in determining that MOST people should be able to (and want to) get on with their pre-COVID normal lives — school, jobs, visitng family and friends, etc (and obviously, making the basic adjustments and precautions for safety)?
In the USA:
1. People under 25 make up 0.13% of COVID-19 deaths … but 32% of the total population.
2. People under 35 make up 0.9% of COVID-19 deaths … but 45% of the total population.
3. People under 45 make up 2.8% of COVID-19 deaths … but 58% of the total population.
4. People over 65 make up 79.4% of COVID-19 deaths … but only 16% of the population!
And remember, even those numbers are muh much smaller when you consider only those w/out underlying health conditions.
Here is where I got my numbers:
https://www.cdc.gov/nchs/nvss/vsrr/covid19/index.htm
https://www.statista.com/statistics/241488/population-of-the-us-by-sex-and-age/
It is provisional data, the numbers are rough, but the final percentages will almost certainly be very close to these. You have to do some math (a spreadsheet helps) to get the percentages on the age breakdowns on both sites.
Young people are suffering from strokes and other sequelae of clotting. They are not part of the mortality statistics but they may be permanently disabled. A Broadway actor who is young had his leg amputated. Most experts think that deaths are being undercounted. That said, I do not believe we can keep the country on lockdown indefinitely. As we get more PPE and testing people will be able to return to work. There are plans to reopen in some of the earliest states to suffer from Coronavirus. Meat processing plants need to modify their production models or workers will not show up regardless.
Thank you, Byron. Certainly a tragedy for the actor and his loved ones. Can you provide links to sources that show statistics in this category? Anecdotes don’t really get to the issue, but statistics do.
To extend my example about car fatalities and kidnappings: I also don’t live my life in fear of getting seriously injured as I drive to work, or my daughter getting severely beaten up on her way to school — even though those types of things DO happen to people and it IS tragic. Again, it is so unlikely that it doesn’t paralyze me into fearful inaction, but I do take reasonable safety precautions for both.
Here is one article I could find. It doesn’t have any reliable statistics, but it reinforces the vulnerability of the elderly, this time to long-term effects rather than death:
https://www.healthline.com/health-news/what-we-know-about-the-long-term-effects-of-covid-19
“Not everyone who beats COVID-19 has the same risk of experiencing long-term consequences from the SARS-CoV-2 infection.
Those most at risk are ‘people 65 years and older, people who live in a nursing home or long-term care facility, people with chronic lung, heart, kidney and liver disease,’ said Dr. Gary Weinstein, pulmonologist/critical care medicine specialist at Texas Health Presbyterian Hospital Dallas (Texas Health Dallas). Additionally, he said others who could be at risk are those with compromised immune systems and people with morbid obesity or diabetes.”
Solid post. Wish more physicians (I am an MD, MBA, MHA) were this rational. They interpret Do No Harm as Do No CLINICAL Harm (or I might get sued). The problem is the cure is going to be worse than the disease. When we pile up the suicides, the depression, the malnutrition, the hopelessness, the lack of an economic future for people graduating into this mess (and so on and so on) this is going to prove to be a low point in the cost benefit of science argument. As someone who spent 10 years in industry I get the reality of things far better than many of my peers who have no experience outside of healthcare.
[…] measures on public health. The situation is bleak, and illustrated by the infographic below. In another piece on his blog, Mandrola discusses the shifting meaning of “flatten the curve,” and makes a point that […]
[…] Can We Discuss Flatten-the-Curve in COVID19? My Eight Assertions, John Mandrola, MD […]
Excellent analysis from my lay person point of view and good advice to the elderly grandparents: take precautions but there is no advantage to waiting for family visits or living in isolation for 18 months.
One major point you did not consider is that we just don’t know what Covid-19 will do in the fall or through the coming winter and spring. Historical records for the Spanish flu indicate that the second wave which hit in the fall of 1918 was much deadlier than the first. Allowing the virus, which may mutate and affect more demographics, to maximize its spread through the summer by lifted social distancing restrictions and opened businesses could be a disaster. Could you address this question, please?
[…] 3. The next pointer is to John Mandrola, MD. […]
You mention that the safety requirements for a vaccine are very high because the fatality rate is very low. This is true if you look at the population as whole, but among the elderly >80 and certain other groups, the fatality rate is something like 20%. I expect an ’emergency use’ vaccine administered to such vulnerable people while not authorized for the general public, followed 6-12 months later by one that’s overcome the higher safety hurdles required for everyone else.
Regarding the slowdown in non-critical medical care, I have a friend who is a radiologist and she is seeing a higher proportion of initial cancer diagnoses at stage 4 because people are waiting until they are quite sick to get checked out. That will cause additional deaths, but they will be 6-months to 2 years in the future.
These are all valid points however they miss an important consideration. Even if no vaccines or treatments are developed in the next 18-24 months and the same amount of people end up dying by Dec 31 2021 “flattening the curve” allows most of these people to live longer than they otherwise would. Which seems to be most of what modern medicine is about, there is no such thing as “saving” someones life only prolonging it. Consider how much is spent annual to increase the life of seniors by a few more years.
That’s why “modern medicine” shouldn’t be the only factor driving the decisions. There should be an analysis of how badly the actions taken will hammer the economy and how many deaths will result from that.
Letting lots of people live a couple extra years longer here and now, at the expense of causing lots and lots to die several years ahead of schedule in the future, is horrible policy.
But somehow, we only get models and media focusing one way: the worst case direct COVID-19 deaths.
I don’t think the virus can be contained. With a 5-6 day incubation period the shutdown would have ended new cases in quite a bit less time than two months if the lockdowns were effective. They aren’t and they are economically and socially destructive.
Has the curve been flattened or is this the curve we would have had without the lockdowns? Folks are passing off “lockdowns are effective” without really any evidence that they are. There is contrary evidence in places that have not locked down.
Sweden is the common example and lockdown supporters point out that Sweden’s numbers are worse than lets say Germany but they fail to acknowledge that they are much better than Italy or Spain.
In a complex process if a variable, like lockdown or no lockdown, does not directly correlate to the outcome it may be a “don”t care’.
But is a quite a concern in regards to economic and social health.
The most important part of your post is the statement that there is no proof the lockdowns did any good. With a number of sources raising the question that the lockdowns increased mortality with elderly (in nursing homes and living with younger family members), it is possible that they caused more deaths..
I have not found a shred of evidence anywhere on earth that asking us to stay home was insufficient to flatten the curve, but making it illegal to go to work WAS sufficient to flatten it.
On the other hand, we have reams and reams of data showing the lockdowns did no good at all. If we can’t see a difference between “please stay home” and “it’s illegal to go to work”, we shouldn’t be worried about going back the other way.
Dr. John,
I believe you need to delete #7. Dr. Faust based his inquiry on his own anecdotal experience as an ER doctor (who would not normally see flu cases – most deaths from flu occur among elderly either outside of hospitals OR admitted through normal channels, not ERs).
Moreover, he clearly does not properly understand the CDC method for estimating flu deaths. He claims that the “fine print” indicates that they co-mingle flu and pneumonia but they only state that they previously surveyed death certificates which include pneumonia as a part of their analysis because flu and pneumonia often coincide.
In fact, “[CDC has] chosen to use a mathematical model that is based on FluSurv-NET, a strong surveillance platform of laboratory-confirmed influenza hospitalizations. We find that the mathematical model is straightforward and can be used to compare one season to another in a way that is simple, yet comprehensive.” https://www.cdc.gov/flu/about/burden/faq.htm
there is a lot to appreciate in your outline but that one just does not belong.
The way to stop deaths is via a vaccine or therapeutic medications. Neither exist. So the only other way is to lock down. We cannot lock down for months or years until a vaccine is available. We can distance and take other mitigating measures to reduce the number of transmissions over time. However, the number of deaths will continue at approximately .04% of the cases. We simply need to ensure the number of cases that require hospital remains below what we can handle.
I agree with what you say, and maybe this helps support it. Something occurred to me that nobody seems to consider: supposing that we get a substantial part of the population tested, what does that mean? Are the people who test negative therefor immune forever? Surely not. So how much re-testing is needed? When will all of this end?
John, I appreciate your very well researched comments. So much of what you are saying is not consistent with “community standards” and if posted on a YouTube video would be deleted. Switzer has excellent questions. The problem with most of what has been done has been rather arbitrary which makes one distrust the “expert” recommendations. How is it that the virus knows the difference between a hardware store and a hair dresser, a Publix from a Popeye’s, a New York or Chicago Mayor and an ordinary citizen. For sure there are risks in every thing we do. Your reasonable request for reliable information falls on deaf ears. All news is fake. there is always an agenda. Americans weigh risks and benefits daily and are perfectly capable of doing this during this pandemic. Your couple stated this nicely. They wanted something reliable. One slight criticism is your graph showing the “capacity of our hospitals”. This estimate is based on a static model. Our healthcare system is the largest, most sophisticated, well stocked and innovative system in the world. New York was provided with 3000 beds and 40K ventilators within days. In the words of Ronald Reagan, there is no problem that can’t be solved by a people who are free to pursue their dream and the profit motive. If we had unleashed the infinite creativity of the human mind and the Yankee Ingenuity that won WWII and many other victories this Pandemic might be over by now. From what I have seen and what you so nicely show in your graphs is the pandemic is actually the panic.
thanks again for your efforts.
all the best to you.
New York Gov. Andrew Cuomo (D) disclosed Wednesday that a recent survey found a “shocking” 66% of the coronavirus patients recently admitted to hospitals in the state are people who became infected despite largely remaining in the their homes during the ongoing outbreak. 18% of the people came from nursing homes, less than 1% came from jail or prison, 2% came from the homeless population, 2% from other congregate facilities, but 66% of the people were at home, which is shocking to us.” Overwhelmingly, the people were at home. We thought maybe they were taking public transportation, and we’ve taken special precautions on public transportation, but actually no, because these people were literally at home.
Do you have a cite?
Highlights the extremely high contagious character of this virus. The people were largely removed from social interaction but got the virus somewhere from someone.
The one good news is that we know now who is most susceptible to severe consequences. These people, myself included, must be vigilant.
Thank you for this enlightening article. I think you clearly articulated what most of us are thinking. Another point to add to your seventh assertion: We should be careful when comparing the IFR of COVID-19 to that of the flu. We need to remember that we have already developed an effective vaccine for the flu. So when people say that the flu kills 0.01% of The US population every year (on average) they forget the fact that a vaccine exists to prevent that. So is COVID really any more deadly than the flu or is it roughly the same but we lack a vaccine? Perhaps we ask the question: what if you we unable to get a flu vaccine this fall? Would you be worried for your life? Food for thought…..
What about the impact of the lockdown and associated economic damage caused to the US and world economies by the lockdown and other measures?
People in shantytowns, squatter camps, favelas, etc all over the world live in subsistence conditions. Before all this many were only just getting by. Now they have nothing… children are starving, malnutrition is rife. I have friends in Africa – they tell me about people eating newspaper just to have something in their stomachs to ease the cramps, they tell me how people are giving their kids three cups of tea per day instead of meals because they have no food, they tell me of how people stood in lines almost 3 miles long to get food parcels worth less than $10
Their governments can’t send them $1,200 checks, can’t pump up their unemployment insurance. They’ve been living hand-to-mouth and have no savings to fall back on.
Opportunistic diseases of poverty will bloom, cholera, tuberculosis, plague, dengue fever, etc…
Yes they’ve been in a bad way for decades, but their conditions were improving – now we have gone and made them far, far worse.
Frankly I believe that Sweden had the right idea, but politicians have so much ego invested in the current situation that they will never hear them admit that they were wrong.
Instead we see them doubling-down.
I agree with all the points except (3) where you say we can ensure hospitals are not over-run. I don’t know mathematically, how to check that.
Secondly, I think you did not stress enough on the bias that #positives and #deaths / # positives has which people focus in. It is so critical, that we focus on # of hospitalization instead. It is not too late as # deaths and not biased by how many and who was tested.
Jayesh, Unfortunately you have to go state by state for utilization rates. Illinois (currently a hot spot) has pretty easy way to look http://www.dph.illinois.gov/covid19/hospitalization-utilization If you look at all states you can start here https://covidtracking.com/data
The COVID tracking folks are trying to get total hospitalized for all states and to have a “current” # . I live in Colorado where there are 792 hospitalized out of 2919 total during the infection. To give you perspective, we have around 12,900 total hospital beds.
Dr. John –
Thanks for the post. Great to see so many thoughtful replies, regardless of whether one agrees with them. Obviously, none of us really know how this will play out, and I am probably particularly under-qualified relative to the credentials of others to make those sorts of predictions. That being said, I have a background in economics and work in the healthcare sector, so, I’m at least topic adjacent. What has always concerned me about the lockdowns in the U.S. is that they have lacked the uniformity, duration, or severity to truly limit the spread of the virus. When we couple that with Americans’ value of personal liberty over public welfare, we were never going to be able to contain this pandemic. Your assertion #1 that the virus will never be contained was probably always true. The best case was to flatten the curve. Your assertion #4 that American’s aren’t stupid probably overestimates what “average” intelligence (of any nationality) is and how easily human opinion and behavior is manipulated.
What was the impact of the lockdown? We slowed transmission, allowed our healthcare system to brace itself for “The Surge”, learn a bit about treatment, created a tremendous amount of fear of the healthcare system, and cratered the economy. The hospitals are relatively empty, we have failed to postpone death from many otherwise treatable diagnosis, and succeeded in postponing deaths from C19. The current death rate is unquestionably higher than normal, but we will never really know what the “optimal” course of action should have been.
In about 12 months we’ll have a real sense of what the real cost in lives of the pandemic has been and with 20/20 hindsight people will judge the actions of today’s leaders from a lens of lost jobs and/or lost loved ones. The die is cast. We have abandoned the lockdowns and debate is fruitless. It could be 200,000 dead or 1,000,000 dead. Tough to turn back now.
What has been enlightening and terribly disturbing for me through this has been how much it has highlighted how little we care for our elderly and vulnerable. How many times have we seen it written that this is really a problem for the old and infirm, so “we”, the non elderly and infirm, should be able to go about our business. Let’s just protect “them”. The problem with that theory is that it is “us” that have to take care of “them”, and if we don’t protect “us”, we can’t protect “them”.
As Mark S. points out above ” People over 65 make up 79.4% of COVID-19 deaths … but only 16% of the population!” and “Shouldn’t THAT be a huge factor in determining that MOST people should be able to (and want to) get on with their pre-COVID normal lives — school, jobs, visitng family and friends,” (Sorry Mark, this isn’t to single you out, you just had the type of quote I was looking for. This is a pretty standard opinion of the situation)
Well, people over 65 are frequently very active and valuable members of this world we live in. They live and work right next to us. Even those that are “past their prime” have value in their life. It isn’t like everyone over 65 is in some sort of institution where they are cared for 24/7. Some are, but that doesn’t mean their lives have no value or that they don’t deserve our respect for what they have given to us as parents/grandparents/friends/mentors/veterans. The caregivers for that group do not live in the same bubbles of assisted/independent living and skilled nursing facilities that they work. So, exposing them exposes the most vulnerable.
So, where do you go with that older couple you mentioned? If I were them, I’d be focused on that long-term goal. I’d shelter from the outside world until there was a vaccine. Get optimistic and its 12 months away. Get it later and treatment will likely improve. Have some faith in modern science. If you get to the vaccine or “herd immunity”, you may see that grandchild graduate high school, or college, or get married, or have kids. People endure greater damage from chemo on less likely outcomes. If they roll the dice, make sure they know the real risk is that if they catch it, X in 10 times they won’t make it.
Please either delete or edit my comment. I made a typo and can’t change it. Thank you.
Social distancing will certainly work.
It HAS worked, quite well, I think.
But can we keep it up for as long as necessary? No. So we will have to deal with the other concept – the ‘hammer and the dance’. This initial shutdown, and then pulling back as things get objectively worse. If we completely give up, given the exponential nature of pandemics and the fact that the vast majority of people in the US have not been exposed will lead us back to having to clamp down.
But keeping some degree of social distancing – universal mask wearing may help – will allow us to keep this pandemic at manageable levels until therapies that help will decrease the death and morbidity rate. Not one magic bullet, but maybe a combo of antibody therapy, recovered victims serum, better anticoagulation, remdisivir, maybe even HCQ, will lead this to become less deadly until we get a vaccine in a year or so. That’s the goal.
You have the right of it, mostly, Very succinct analysis. The bottom line is this: We must learn to live with this disease. We cannot stop it in the short term, we cannot live with the economic damage in the long term.
I met an ER doc one time, and he was convinced that circular saws were the most dangerous thing ever because of the steady stream of patients he saw who cut off finger tips. What he DIDN’T see were the zillions of people of did NOT cut off their fingers with circ saws. LIkewise, all these doctors and epidemiologists hyperventilating about Covid deaths are not economists, businessmen, or single mothers. They see the patients on ventilators clinging to life, but not the misery of the economic devastation foisted on MILLIONS of people due to the lockdown. The suicides, drug addictions, domestic abuse and general misery caused by anxiety and financial ruin.
So, my only quibble with this piece is this: it does not make sense to stay locked down even for one year. Even if that meant the virus would be exterminated (and it won’t be). In one year of lockdown, the resulting societal damage would dwarf the damage caused by the virus. We have to get some perspective on this, see the bigger picture.
[…] to get involved in the political circus of flattening the curve and social distancing. I read an article today by a cardiologist, John Mandrola M.D., which most accurately represents my thoughts on the […]
Making a list of objections/corrections as I read through:
1. “Once-in-a-lifetime situation”? Whose lifetime? It’s not at all unlikely that a situation like this will recur in the next 20, 40, 60 years.
2. NYC hospitals *were* overwhelmed, and people (including healthcare workers) died as a result. Rural hospitals will be overwhelmed in places that are refusing to lock down. The US as a whole is NOT in the blue part of the curve. “Flatten the curve to prevent overwhelming healthcare” is not obsolete in the US, because:
3. “Flatten the curve” was also about improving the ability to test, trace, and contain while locked down. NZ did that. The US did not, still is nowhere near doing it.
4. “The virus will not be contained”: globally, no. Locally, yes. NZ may well have contained it. Taiwan as well. Regions of the US that have seen only a few cases so far could still do it. But they’re not.
5. “We should expect less from test and trace”: there are problems with tests, but not all tests are equally bad. The ones the US has been determined to use seem to be particularly bad. In less fucked-up countries. test and trace has worked well.
6. No doubt some hospitals in the US are prepared. Some are clearly not. “I’ve talked to numerous colleagues in the US” who say hospitals are plenty prepared is not evidence of anything about the US as a whole. (And, yes, a fucked-up healthcare system means hospitals can go bankrupt when they can’t charge big bucks for elective procedures. Hi, your healthcare system is fucked up.)
7. “Americans are not stupid”. Give me a fucking break. We have copious evidence to the contrary every day. And if you think it’s OK if only a sizeable minority is out there infecting people, then you don’t understand how infectious disease works.
8. “Public health surveillance has improved” (with useless-but-not useless testing): Seriously? The US has one of the lowest per capita rates of testing while having more cases and deaths than anywhere in the world. Oh, yeah, I’m sure a resting heart rate app (oh, look he’s a cardiac electrophysiologist) is going to be a game-changer.
9. “Due to the contagion of this virus, the area under these curves is likely to be the same at the end of two years.” LOL. You know what? That depends entirely on whether or not you have COMPETENT PUBLIC HEALTH POLICIES. Which is supposedly what you’re arguing about. So you’ve just assumed the outcome you’re supposed to be demonstrating.
10. “the basic math of COVID19 creates a huge barrier for success: already, more than 99% of people infected with this virus survive. A therapy that has a massive 50% reduction in death from a disease with 1% mortality (high estimate) delivers only a 0.5% absolute risk reduction”– 50%of 3million people is 1.5 million people. Inconsequential?
11. “This preprint from prominent researchers suggests a substantial proportion of excess deaths observed during the pandemic are not attributed to COVID19 and may represent an excess of deaths due to other causes.” This is worst-faith point so far. You know which deaths are attributed to Covid-19? The ones where people actually managed to get tested. You know what proportion of people managed to get tested in NYC? A tiny one. It is impossible to read the first-hand accounts of EMTs in NYC and not realise that a huge number of people died at home because of Covid-19 but were never classified as C-19 because NYC was too overwhelmed to test dead people.
12. “COVID19 interventions … make poor people even poorer”: You know what the answer to that is??? POLICIES THAT ADDRESS POVERTY. i am very curious to know how many of the people making the point that lockdown is bad because it hurts poor people have EVER in their lives advocated for policies that would improve the lives of poor people.
Finally, a general point. Why is this being treated as binary choice? “Flatten the curve” is being equated here with some meaning of “lockdown” (which meaning, who knows, because in the US it is chaotic), and you’re either in it or you’re not. Intelligent governments have phased approaches. Lockdown until a certain level of control is reached, and then gradually phasing out restrictions WHILE MONITORING CLOSELY TO ENSURE THAT OUTBREAKS CAN BE ISOLATED. Again, NZ is a good example. This article shows no awareness of this strategy. Or just implicitly assumes the US is not capable of it. In which case, why the fuck are you not talking about why the US needs to get itself capable?
Maybe losing the f-Bombs would make your case better. Right now you seem just to be ranting and raving. Fortunately we are not NZ.
Sweden’s curve of death is actually coming down. Not because they shut down, but presumably because immunity is starting to kick in. There will be no second wave in Sweden because they never shut down. The health minister predicts that 30% of Stockholm already has the antibodies. As of yesterday Sweden had 291 deaths per million, the US 218. The difference is 30% of Sweden has antibodies and maybe 5% or 10% in the US.
And in time it will be obvious that Sweden made the right decision while the rest of us are still living in fear. They took the bandaid off quickly, we are doing it slowly. Bandaid must still come off either way.
Important details you failed to mention:
New Zealand has a population of approx. 5 million people living in a land mass of 101K sq. miles and most of the people 87% live in urban centers. Their biggest urban center is about 1.5 million people. See: https://en.wikipedia.org/wiki/Urban_areas_of_New_Zealand
The US has about 327 million people living in a land mass of 3.8 million sq. miles. The US has individual cities, not to mention states, which are multiple times larger than the country of NZ.
Implying that the two countries have the same logistical challenges is absurd. Getting angry about it is insane.
Thank you for your usual thoughtful and provoking commentary. This is such a confusing time for patients as we don’t have the skills to weigh conflicting ideas and advice from medicine. However, my skills have been honed by you! Having listened to your podcasts and read your blog, I’ve been trained by you to look for conflicts. So, as a patient, I’d love for you to discuss whether any of your thoughts here may be influenced by the reduction in income for most of medicine.
Lock downs for younger people (under 65? under 50?) are likely more harmful than beneficial. In the instance of children, in particular, denying their developing immune systems the natural recurring challenges in their environment may be setting them up for serious illness later.
One compelling theory of the virulence of the poliomyelitis epidemics in the mid-20th century was the effect of late 19th century sanitation efforts. The effect of that progress was to remove the polio virus from its prior normal encounters with children, allowing them to have a mild form of the disease and create antibodies. Over several generations, all population immunity was lost so when the disease came back it was particularly harmful.
Combine weakened immune systems with deliberately partially shutting down the hospital system to create reserve capacity and we may have created a perfect storm – another opportunistic disease challenging our hospitals’ abilitity to surge in response to it.
Why aren’t the government and the scientists just telling us what we should be doing to strengthen our bodies defenses? Stop disinfecting your home, get plenty of exercise and sleep, take vitamins, and eat well. Combine those with wash hands frequently (especially after returning home), socially distance, and wear a mask in public situations. Then know your own level of vulnerability (age, overall health, co-morbidities) and own the responsibility to take measures that are appropriate.
I am concerned more lockdowns will ultimately bring inter-generational conflict, beginning with the obvious but unstated question, just who are we all going to this trouble and expense to save?
What is being overlooked in general is that we get so wrapped up in dealing with the effects that we ignore what we can do to prevent the problem, which is reading a healthy diet to support our immune system. So the logical strategy is both to do whatever you can to prevent overwhelming the health system in the short run and to help people to prevent or reverse as much as possible the comorbidities which are the real problem and which are all caused by our bad industrial diet.
With regard to the elderly couple’s question, you seem to skip over one important fact. Time doesn’t make the virus less dangerous, but it DOES decrease your risk of catching it. Every day, more people recover and presumably cannot infect anyone else.
This is why shutting down the economy could cost even more lives. My 86 and 85 parents are in quarantine since the beginning of March. They are willing to cooperate for a few months but not 18 months without their grandkids. We are all going to follow Sweden’s lead at some point. It is a shame we could figure out to protect those in nursing homes, including Sweden, from the beginning.
That is precisely why we need to fully open now – concerts, theaters, restaurants, etc. Shorten the time until we have the ‘herd immunity’ you suggest.
You guys are missing the point. You can’t have one without the other. If you open everything up, everyone gets infected. You’ll have “herd immunity” but at that point there will be hardly anybody to protect. It needs to be a balance.
The virus is upon us. Short of a vaccine, the reality that COVID-19 will kill some people under certain conditions is unavoidable. Most Americans (self included) supported the initial shut down so we could flatten the curve and give the hospitals time.
The truth is, lockdowns have differential effects for different people. At some point, the law of diminishing returns kicks in for the majority who will not/would not die from it. I believe we are at that point. Asking society to wait for months and months for treatments or a vaccine that may or may not reduce mortality rates is both illogical and unfair.
Leaders should be saying, “Folks, there is a virus. Most all of you will get it and survive. Some of you will be hospitalized. Some of you will die from it. Short of a miracle, we will not eradicate this virus within 2 years. Everyone staying home is as detrimental to economic, mental, emotional, and physical health as people living their lives and being exposed to COVID-19.â€
Gradual re-openings coupled with practical advice for vulnerable populations continuing to self-monitor and shelter will help ensure hospitals don’t get overrun.
But this strategy of pitting daily counts of COVID deaths against every other present & future societal good isn’t working.
Jessica, You are obviously a rational person.so few these days.
I agree except for one thing. I don’t think the reopening needs to be gradual. As you say, you will be exposed eventually unless you stay inside for 2yrs or…whenever. The sooner we get the ‘working herd’ immune, the safe it is for those who wish to isolate, etc., to venture forth, and even be safer in their own homes. If we fully open now, we can possibly have significant immunity before this fall/winter, which can help save the home-dwellers.
Not even counting those lives that are dead/negatively affected by the lockdown, we will save moralizes than we cost by opening immediately.
I am fairly high risk due to age (60) and very bad asthma. I have been intubated without any viral involvement. My doctor’s guess is that I have 40% of normal lung capacity. I do not have COPD or a poor immune system. So…
I actually do take some comfort from the fact that the longer I can hold off getting Covid, the better medical care I may get. I do not expect a miracle drug, but know that doctors are building understanding of the best /safest supportive care each day.. I will be more cautious than some, but still think we should reopen the economy in stages as long as crazy infection spikes like what happened in NYC don’t occur. Even then, it would be a localized problem.
The damage is too great to mental health and lower income communities to continue lockdown.
Do you have any statistics about this?
Early COVID19 surges were over-running some big-city hospitals. This was bad because it caused excess or preventable death–people who could have been saved were not saved because of shortages of ICU beds, dialysis equipment, staff and ventilators.
Early COVID issues in NYC and New Jersey were restricted to a few hospitals 4in New Jersey full hospital overload and 4 additional ICU’s in New Jersey(from New Jersey’s site). New York appeared to be a dozen or so hospitals. In both cases a simple transfer of patients to other available hospitals would have solved the issue. But due to restrictions on ambulance travel, contracts to bring patients to certain hospitals, hospitals wanting the revenue, not willing to transfer to other hospital chains and other bureaucratic issues, there was not a “sharing” of patients. Gov. Cuomo had several slides on this at the end of March briefing. Other than a few rural hospitals and 2 in New Orleans for two days, the loads have not been close to capacity. For example California currently has 4,681 COVID patients hospitalized now and has 128,000 licensed beds. https://covidtracking.com/data The issue has never been capacity of the overall system, but capacity of a few hospitals. Restrictions make it harder to even out the patient flow. You might think this is a US only issue, but it happened in Italy and Spain. In France they made special COVID trains to even the load from Paris around the country. https://abcnews.go.com/Health/wireStory/france-turns-speedy-trains-catch-virus-response-69982731
[…] Doc John discussing whether it makes sense to flatten. John has credibility with me because: (a) when he writes about niches I know very well (exercise), he makes sense; and (b) he’s willing to share observations that work against his financial and business interests. […]
[…] writes another column questioning the notion of flattening the curve by extensive lockdowns. Â Â (Column)Â Â His basic point is that flattening the curve isn’t saving lives at this point, it is just […]
The safer at home or shelter in place measures we’re practicing now aren’t sustainable, as the need for interaction for overall health is fundamental. As May is mental health awareness month, the tension between the need to isolate for COVID-19 and the need to NOT isolate for anxiety and depression is brought into clear focus. For people with pre-existing mental health issues (1 in 4 adults in the US), extended isolation is an attack to what is already a difficult chronic diagnosis to manage, and further exacerbated by online (if they have access) therapy only, and the closure of faith organizations, both of which are important mental health management tools. I have not yet seen data comparing suicide rates for March and April 2019-2020, tho anecdotal observation and what we know about mental illness suggest an almost certain increase.
I don’t know the answer, but agree we need to be thinking about a long-term lifestyle with appropriate safety built into a new interaction pattern.
Thank you for posting and for your invitation to share thoughts, opinions and questions.
I am annoyed by Dr Faust’s comment that it was okay to intentionally overestimate flu deaths to encourage vaccination. The flu vaccine is not effective. Multiple Cochran meta anayses could barely find any benefit, in spite of the fact that many of the studies were funded by industry and designed to have good outcomes. And there are risks like GBS. Tell us the freaking truth so we can decide for ourselves.
What he’s saying is basically, it was cool to lie about flu deaths to scare people into getting a vaccine (that almost definitely won’t do anything), but it’s really backfired on us now.
Wow! You are the first medical professional to say what I’ve been thinking all along. I’m not a doctor, but I can do the math. I’ve been so angry at politicians using the flatten the curve phrase to say the isolation is reducing the number of cases.
Thank you for articulating the math so well!
I don’t want to see people get sick or die, but I also don’t think living in isolation ‘for the foreseeable future’ is living.
We need to meet in the middle on the debat, sooner rather than later.
Thank you for this great article. You say exactly what I’ve been thinking, but haven’t known how to say. It’s courageous for you to express these ideas. It seems like anyone who questions the groupthink is labeled as simply selfish, stupid, arrogant, etc.
I will go one step further. Selfish applies to the lockdown people. Virtually every politician, most government employees, and everyone living on social welfare benefits including Social Security, and pensioners are all getting paid. They may be inconvenienced, but they are not going broke. In fact, many of them are making more money than they used to. If everyone of these people had to sacrifice their income, including wealthy people sacrificing theirs as well, this lockdown would end in five minutes.
Their holier-than-thou attitude is hypocritical at best.
[…] doctor’s thoughts on flattening the […]
[…] physician’s ideas on pulling down the […]
[…] doctor’s thoughts on flattening the […]
[…] doctor’s thoughts on flattening the […]
[…] doctor’s thoughts on flattening the […]
This is the most thoughtful, non-politicized, rational discussion of the topic I have seen. Thank you. Mc
[…] physician’s thoughts on flattening the […]
[…] doctor’s thoughts on flattening the […]
[…] doctor’s thoughts on flattening the […]
[…] doctor’s thoughts on flattening the […]
[…] doctor’s thoughts on flattening the […]
[…] doctor’s thoughts on flattening the […]
[…] doctor’s thoughts on flattening the […]
[…] physician’s ideas on flattening the […]
[…] physician’s thoughts on flattening the […]
[…] doctor’s thoughts on flattening the […]
[…] doctor’s thoughts on flattening the […]
[…] doctor’s thoughts on flattening the […]
[…] physician’s thoughts on flattening the […]
[…] physician’s thoughts on flattening the […]
[…] doctor’s thoughts on flattening the […]
[…] doctor’s thoughts on flattening the […]
[…] doctor’s thoughts on flattening the […]
[…] doctor’s thoughts on flattening the […]
[…] doctor’s thoughts on flattening the […]