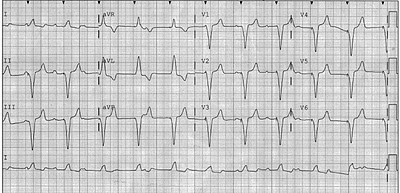
The case involved a 70 year-old man with an eight year-old medical device. He suffered the abrupt onset of chest pain and shortness of breath. His ECG is here:
 |
| Click to enlarge |
The Answer:
First, the ‘medical device’ is an eight year-old Medtronic dual chamber pacemaker.
Second, as was correctly stated, the ECG shows a ventricular paced rhythm. The atria are in sinus, but despite the presence of two leads, there is no evidence of atrial tracking. (Also, RV apical pacing creates a LBBB-like pattern and so the ST-T wave abnormalities are simply the typical reciprocal changes of a LBBB.)
Why would there be a lack of AV synchrony?
It turns out that when Medtronic (only-MDT) dual chamber pacemakers reach a threshold low battery voltage–this used to be called EOL (end-of-life), but now is more politically correctly termed ERI (elective replacement indicator)–the device switches from a dual mode of functionality to one of a single mode (VVI.)
The result is a profound version of Pacemaker Syndrome. The sudden switch from atrial-ventricular synchrony to dyssynchronous ventricular-only pacing not infrequently causes intense cardiac symptoms, including chest pain, shortness of breath and a feeling of doom.
In the last two years, I have seen four cases in which this ERI-behavior resulted in unnecessary diagnostic testing—which in the case of cardiology entails exposing the patient to radiation-laden testing. Two cases were referred for nuclear stress testing and two for cardiac catheterization, before the correct diagnosis was made. Yes, this scenario duped cardiologists.
This is not a zebra case. Medtronic approximates that there are 250,000 patients with MDT-branded dual-chamber pacemakers (personal communication), and all will exhibit this behavior when their ERI-threshold voltage is reached.
Personally, I have never understood the reasoning for such dramatic signaling that it is time to change the pacemaker generator. Two of the other major pacemaker companies have programmed much more subtle means to signal generator-replacement time.
I asked Medtronic for an explanation and received this:
“VVI 65 has been our ERI/RRT operation ever since we have had dual chamber devices.
This mode and rate were seen as a safe compromise operation which provides a more predictable ERI to EOL service life and an easily identifiable indicator via trans-telephonic monitor or surface ECG/EKG strip.
There are arguments in both camps to change this and to leave it as is. However, new industry standards for magnet operation and ERI/RRT indicators will soon replace this operation with something else. You will be getting these details as they are developed into our newer generation products.”
So things may change in the future.
But for now, the dogma which says that a paced rhythm on an ECG precludes making a diagnosis is not true.
Sorry to complicate the diagnosis of chest pain, but when a pacemaker is present, and there is asynchronous pacing, consider end-of-life (ERI) pacemaker behavior as a potential cause.
In this case changing the pacemaker generator did indeed alleviate the symptoms.
Thanks to all those who offered their diagnosis.
JMM
Disclaimer: I have no financial interests in any of three major pacemaker companies. I use all three companies. They each have their strengths and weaknesses.
3 replies on “An answer to this week’s clinical vignette”
This was fun. Hadn't heard of that before. Thanks.
Is there a registry of who received these devices, and perhaps when? Would it be possible to notify these poor souls of what is about to happen to them so they could alert their doctors? If you had described this scenario for alerting end of life on a battery I would have believed your were joshing me.
Thanks, Steve.
AM,
It has been this way since the 1970's, and then, this mode-switching behavior was probably a good idea. Presently, we have far more advanced monitoring capabilities and the likelihood of a pacemaker getting "lost to follow-up" is quite low.
But MDT seems to have been "busy" with developing other technologies and this archaic modality was left in place.
We do our best to alert patients to this inevitability. But not all get told, or remember. And many patients have only mild symptoms.
Joshing you, no.
Like the MDT spokesperson said, hopefully industry standards will push this nonsensical modality into extinction.
JMM